Systemic Lupus Erythematosus
Updated: 11/25/2016
Although Rheumatology falls under the Orthopedics section of the PANCE, which counts for 10% of the test, it isn’t heavily emphasized during PANCE review courses or in PA school, for that matter. I think our program probably spent 1 week or less on Rheumatology. This part of the test doesn’t have to be scary and it doesn’t have to be a bunch of memorization, either. Just remembering the basics can get you the answers you need to a few questions on the PANCE so that you’re not missing the easy “quick and dirty” questions.
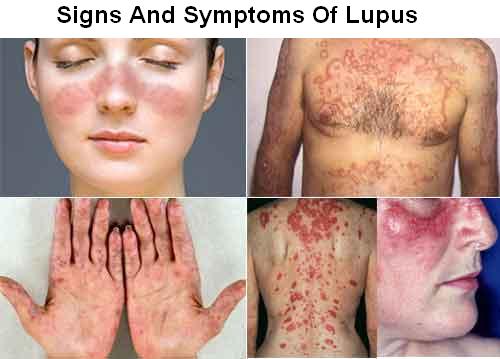
A good place to start is with lupus. Lupus is an autoimmune disease that can affect many systems and one of the most challenging aspects about diagnosing it is that many of the symptoms are nonspecific and overlap with other common conditions. You’re almost guaranteed to have a question or two on lupus on your PACKRAT, EOR Exam, PANCE or PANRE. The thing to note about all rheumatological conditions are their overlaps and subtle differences. Lupus has a very characteristic malar rash that is often tested over - keep in mind they can give you a description or photo with a corresponding vignette. Don’t focus too much on all of the manifestations of lupus. It can appear quite vague most times and is often a diagnosis of exclusion.
Oftentimes, you’ll find that they give you or ask you about serological markers for various rheumatological conditions. This is where some memorization might be needed. Knowing which markers are most SENSITIVE and which are most SPECIFIC and what that means will aid you in your diagnosis.
Lastly, know the treatment for lupus and the adverse effects of the medications, which I’ve provided below. Ask yourself - what would I need to monitor in a patient taking Plaquenil and how often? I have yet to see any questions on newer medications for lupus. Most ask about acute therapies and chronic therapies - just know the difference between them and how they are used to alter the progression of the disease. You might also want to be familiar with the mechanism of action for medications - although not often tested over, questions like this will come up.
Systemic Lupus Erythematosus (SLE)* - an autoimmune disorder leading to inflammation and tissue damage involving multiple organ systems
- Genetic, environmental and hormonal factors involved
- Autoantibody production, deposition of immune complexes, complement activation, and tissue destruction/vasculitis
- The incidence of non-Hodgkin lymphoma is increased three- to fourfold compared with the general population
- Increased risk of cardiovascular disease
- Types of Lupus
- Spontaneous
- Discoid lupus (skin lesions, no systemic disease): erythematous raised patches with keratotic scaling
- Drug-induced lupus
- ANA-negative lupus
- Arthritis, Raynaud’s phenomenon, subacute cutaneous lupus
- Serology: Ro (anti-SS-A) antibody (+), ANA negative
- Risk of neonatal lupus in infants of affected mothers: skin lesions, cardiac abnormalities (AV block, transposition of great vessels), valvular/septal defects
- Clinical Course
- Chronic disease with exacerbations and remissions
- Malar rash, joint pain & fatigue
Systemic Lupus Erythematosus (SLE)
|
Women of childbearing age (90%)
African American
More severe in children
Appears in late childhood or adolescence
|
1. Constitutional SX: Fatigue, fever, weight loss
2. Arthralgia, myalgia
Manifestations
2. Skin: butterfly rash over cheeks and bridge of nose (⅓), photosensitivity (23%), discoid lesions, oral and nasopharyngeal ulcers, alopecia, Raynaud’s phenomenon (16%)
3. MS: joint pain (90%), arthritis (symmetric), arthralgias, myalgia +/- myositis
4. Cardiac: pericarditis, endocarditis, myocarditis
5. Lung: pleuritis (16%), pleural effusion, pneumonitis
6. Heme: hemolytic anemia with anemia or reticulocytosis of chronic disease, leukopenia, lymphopenia, thrombocytopenia
7. Renal: proteinuria >0.5 g/day, cellular casts, GN, azotemia, pyuria, uremia, HTN
8. Immune: impaired response due to autoantibodies to lymphocytes, abnormal T cell function, and immunosuppressive meds
9. GI: nausea, vomiting, dyspepsia, dysphagia, PUD
10. CNS: seizures, psychosis, depression, headaches, TIA, CVA
11. Other: conjunctivitis, Sjogren’s syndrome
|
1. (+) ANA screening: sensitive, not specific
2. Anti-dsDNA (40%) and anti-Sm Ab (30%): not sensitive, very specific
Other Antibodies
Anti-ss DNA (70%)
Antihistone Abs (70%) in 100% of drug-induced lupus (Ro 9SS-A) and La (SS-B)
(+) LE preparation: ANA binds nuclei of damaged cells, producing LE antibodies
False (+) syphilis
Complement: decreased
3. CBC, BUN/Cr, U/A, serum electrolytes
4. Anticardiolipin and lupus anticoagulant
|
Acute
1. NSAIDs if less severe
2. Local or systemic corticosteroids
3. Systemic steroids for severe manifestations
Chronic
1. Plaquenil (hydroxychloroquine)
-Annual eye exam
2. Cytotoxic agents (cyclophosphamide)
-For active GN
Health Maintenance
1. Avoid sun exposure, use sunscreen and wear protective clothing
2. Minimize exertion and get adequate sleep
3. Do not give live vaccines while undergoing immunosuppressive therapy
Monitor
1. Renal disease: U/A and SCr every 3 months
2. Hypertension - treat CV risk factors aggressively
3. Monitor and treat infection (especially if leukopenic)
4. Complements, CBC - every 3-6 months
|
Note: The ACR (American College of Rheumatology) and SLICC (Systemic Lupus International Collaborating Clinics) criteria are used to diagnose lupus, however, I have yet to see this tested on any exam. I think the major thing to know here would be that 11 ACR criteria are required for diagnosis, whereas 13 SLICC criteria (including one clinical and one immunologic criterion) are required for diagnosis OR a biopsy confirming lupus nephritis in the presence of a (+) ANA or anti-dsDNA.
Lupus Medications
Medication
|
Indications
|
Dose
|
Monitoring/Precautions
|
Nonsteroidal anti-inflammatory drugs
|
Lupus joint pain
|
Depends on preparation
|
CBC and renal testing annually; use with caution in patients with gastrointestinal bleeding, liver or kidney disease, or hypertension
|
Methotrexate
|
Arthritis, cutaneous lupus, serositis, severe SLE
|
7.5 to 25 mg per week
|
CBC and complete metabolic panel at least every three months to monitor for myelosuppression, hepatic fibrosis, and pulmonary infiltrates and fibrosis
|
Hydroxychloroquine (Plaquenil)
|
Long-term protective effect on SLE-related organ damage
|
200 to 400 mg per day
|
Ophthalmologic examination every six to 12 months to monitor for macular damage
|
Glucocorticoids
|
Low dose for treating SLE without major organ damage; higher doses for cerebritis, lupus nephritis, refractory conditions, and thrombocytopenia
|
|
Glucose levels every three to six months, and total cholesterol level and bone density testing annually; use with caution in patients with hypertension, hyperglycemia, hyperlipidemia, osteoporosis, or infection
|
Mycophenolate (Cellcept)
|
Lupus nephritis, refractory SLE
|
2 to 3 g per day
|
CBC and complete metabolic panel at least every three months to monitor for myelosuppression and infection
|
Cyclophosphamide
|
Lupus nephritis, severe SLE
|
1 to 3 mg per kg per day
|
CBC and complete metabolic panel at least every three months to monitor for myelosuppression, malignancy, immunosuppression, and hemorrhagic cystitis
|
Azathioprine (Imuran)
|
Lupus nephritis, severe SLE
|
1.5 to 2.5 mg per kg per day
|
CBC and complete metabolic panel at least every three months to monitor for myelosuppression, hepatotoxicity, and lymphoproliferative disorders
|
Belimumab (Benlysta)
|
SLE
|
10 mg per kg IV per day
|
Monitor for serious infection and malignancies
|
Rituximab (Rituxan)
|
Refractory severe SLE
|
Two 1-g doses IV, two weeks apart
|
CBC every two to four months; use with caution in patients with history of infusion reaction
|
Below are a few free questions from TrueLearn’s SmartBanks, which are optimized to help you pass the PANCE. Feel free to check their site out if you feel like these were good practice and you want more.
Question 1: A 32-year old African American female presents with wrist pain of 12 weeks' duration. Review of system is positive for fatigue, malaise, myalgias, and morning stiffness. Past medical history is negative for any illnesses except a spontaneous miscarriage. Family history is significant for a mother with rheumatoid arthritis and Hashimoto's disease. Vital signs reveal the following:
Temperature 37.8ºC (100.0ºF)
Blood pressure 100/60 mmHg
Heart rate 70/min
Respiratory rate 16/min
Physical examination is remarkable for mild erythema and tenderness of the third, fourth and fifth metacarpal joints in the hands and wrists bilaterally. Small painless ulcers are noted in the mouth as well. Laboratory analysis exhibits thyroxine 6 ug/dL, erythrocyte sedimentation rate 240 mm/hr, blood urea nitrogen 25.5 mg/dL and creatinine 1.6 mg/dL with trace proteinuria. Plain film radiography of the bilateral wrists display soft tissue swelling without joint space narrowing or bone erosions.
The most appropriate diagnosis is:
A. hypothyroidism
B. rheumatoid arthritis
C. Sheehan's syndrome
D. Sjögren's syndrome
E. systemic lupus erythematosus
Temperature 37.8ºC (100.0ºF)
Blood pressure 100/60 mmHg
Heart rate 70/min
Respiratory rate 16/min
Physical examination is remarkable for mild erythema and tenderness of the third, fourth and fifth metacarpal joints in the hands and wrists bilaterally. Small painless ulcers are noted in the mouth as well. Laboratory analysis exhibits thyroxine 6 ug/dL, erythrocyte sedimentation rate 240 mm/hr, blood urea nitrogen 25.5 mg/dL and creatinine 1.6 mg/dL with trace proteinuria. Plain film radiography of the bilateral wrists display soft tissue swelling without joint space narrowing or bone erosions.
The most appropriate diagnosis is:
A. hypothyroidism
B. rheumatoid arthritis
C. Sheehan's syndrome
D. Sjögren's syndrome
E. systemic lupus erythematosus
Explanation:
This patient's presentation of polyarticular arthritis, fever, renal dysfunction, recent miscarriage is suggestive of a rheumatologic disorder. Given history of miscarriage, antiphospholipid antibody syndrome seen in association with Systemic lupus erythematosus (SLE) is a more likely diagnosis than rheumatoid arthritis. SLE is a chronic autoimmune inflammatory disease characterized by multiple organ involvement. Classic symptoms include fever, malaise, joint pain and rash. Physical examination can present with discoid or butterfly rash with arthritis, glomerulonephritis, pericarditis and endocarditis. According to the American College of Rheumatology (ACR), at least 4 out of 11 criteria must be met for diagnosis of SLE including mucocutaneous manifestations, evidence of serositis and arthritis, renal failure, neurologic manifestations, hematological and/or immunological markers. This patients clinical presentation with oral ulcers, serositis, arthritis, and renal failure is consistent with SLE.
Answer A: Hypothyroidism can also present with weakness, malaise, and myalgias but it does not typically present with arthralgias or renal dysfunction as present in this patient. Typical symptoms include lethargy, weight gain, dry skin, cold intolerance, and constipation. Physical examination can be significant for slow movements, dry skin, coarse hair or hair loss. Diagnosis is made by thyroid function studies, including thyroid stimulating hormone, thyroxine and trioothryroxidine levels. Although she has a positive family history of hashimoto's disease, normal thyroxine values and lack of clinical symptoms make the diagnosis of hypothyroidism unlikely in this patient.
Answer B: Rheumatoid arthritis (RA) is also a chronic inflammatory autoimmune disease like SLE involving the synovium of joints. Initial presentation can be similar to SLE with fever, malaise, weakness along with symmetric polyarthritis. Autoimmune reaction causes joint inflammation, synovial hypertrophy and subcutaneous nodules on the extensor surfaces. Joint and tendon destruction may lead to ulnar deviation, boutonnière deformity, and joint ankylosis. Extraarticular manifestations include pericarditis and valvular incompetence, interstitial fibrosis, and ocular inflammation. However, it does not typically present with renal dysfunction and history of miscarriages as present in this patient which makes SLE a more likely diagnosis.
Answer C: Sheehan’s syndrome is the infarction of the pituitary gland as a complication of postpartum hemorrhage. During pregnancy, the pituitary gland is physiology enlarged and sensitive to changes in functioning. Complications in pregnancy or delivery such as profound hypotension and electrolyte abnormalities exacerbate the gland. Symptoms range from mild to moderate and vary from panhypopituitarism to select pituitary deficiencies. However, this patient only had a miscarriage and does not have a history of significant blood loss which makes this diagnosis unlikely.
Answer D: Sjögren's syndrome is also an autoimmune disease that can present as isolated Sjogren's syndrome or secondary syndrome. Classic symptoms of primary disease include dry eyes, dry mouth and bilateral parotid gland enlargement. Secondary Sjögren's syndrome is associated with other inflammatory disorders such as systemic lupus erythematous (SLE), rheumatoid arthritis, or scleroderma. It can have similar presentation with fever, malaise, fatigue along with chronic arthritis. Hallmark features include dry eyes and dry mouth which are absent in the patient making it an unlikely diagnosis.
Bottom Line: SLE is a systemic chronic inflammatory disease that can be diagnosed based on meeting four out of eleven criteria indicating multiorgan involvement.
For more information, see:
Agabegi S, Agabegi E. Step-Up To Medicine. 3rd ed. Philadelphia, PA. Lippincott: Williams & Wilkins; 2013: 243-244, 246.
Answer C: Sheehan’s syndrome is the infarction of the pituitary gland as a complication of postpartum hemorrhage. During pregnancy, the pituitary gland is physiology enlarged and sensitive to changes in functioning. Complications in pregnancy or delivery such as profound hypotension and electrolyte abnormalities exacerbate the gland. Symptoms range from mild to moderate and vary from panhypopituitarism to select pituitary deficiencies. However, this patient only had a miscarriage and does not have a history of significant blood loss which makes this diagnosis unlikely.
Answer D: Sjögren's syndrome is also an autoimmune disease that can present as isolated Sjogren's syndrome or secondary syndrome. Classic symptoms of primary disease include dry eyes, dry mouth and bilateral parotid gland enlargement. Secondary Sjögren's syndrome is associated with other inflammatory disorders such as systemic lupus erythematous (SLE), rheumatoid arthritis, or scleroderma. It can have similar presentation with fever, malaise, fatigue along with chronic arthritis. Hallmark features include dry eyes and dry mouth which are absent in the patient making it an unlikely diagnosis.
Bottom Line: SLE is a systemic chronic inflammatory disease that can be diagnosed based on meeting four out of eleven criteria indicating multiorgan involvement.
For more information, see:
Agabegi S, Agabegi E. Step-Up To Medicine. 3rd ed. Philadelphia, PA. Lippincott: Williams & Wilkins; 2013: 243-244, 246.
Question 2: A 32-year old African American female presents with wrist pain of 12 weeks' duration. Review of system is positive for fatigue, malaise, myalgias, and morning stiffness. Past medical history is negative for any illnesses except a spontaneous miscarriage. Family history is significant for a mother with rheumatoid arthritis and Hashimoto's disease. Vital signs reveal the following:
Temperature 37.8ºC (100.0ºF)
Blood pressure 100/60 mmHg
Heart rate 70/min
Respiratory rate 16/min
Physical examination is remarkable for mild erythema and tenderness of the third, fourth and fifth metacarpal joints in the hands and wrists bilaterally. Small painless ulcers are noted in the mouth as well. Laboratory analysis exhibits thyroxine 6 ug/dL, erythrocyte sedimentation rate 240 mm/hr, blood urea nitrogen 25.5 mg/dL and creatinine 1.6 mg/dL with trace proteinuria. Plain film radiography of the bilateral wrists display soft tissue swelling without joint space narrowing or bone erosions.
Which of the following is likely additional manifestation of this patient's position?
A. dusty central area with an erythematous halo
B. erythematous eruption on eyelids
C. erythematous raised patches
D. firm lumps next to flexor surfaces
E. silvery white scales
Explanation:
Mucocutaneous manifestations are involved in over 80% of patients with systemic lupus erythematosus (SLE). There are four types of mucocutaneous lesions that are a part of the American College of Rheumatology diagnostic criteria of SLE. These include malar (butterfly) rash, discoid rash, photosensitivity and oral ulcers. Discoid lesions are erythematous raised patches with adherent keratosis scaling which can present on the face, neck, and scalp. Another common dermatological lesion seen in SLE is a malar rash, an erythematous rash located over the malar eminences with sparing of the nasolabial folds. These rashes are generally photosensitivity as they worsen or manifest after sun exposure.
Answer A: A target lesion contains a dusky central spot with a dark red inflammatory zone and an erythematous halo on the extreme periphery of the lesion. A target lesion is the hallmark of erythema multiforme (EM) and is not typical of SLE. EM is an acute, immune-mediated condition induced by infection, medications, malignancy and/or autoimmune disease. These lesions are accompanied by erosions involving the oral, genital and/or ocular mucosa. Nonspecific laboratory analysis include elevated erythrocyte sedimentation rate, white blood cell count, and hepatic transaminases. EM is a self-limiting disease that resolves within weeks.
Answer B: A heliotrope eruption is an erythematous eruption located on the upper eyelids with edema. Gottron's papules are erythematous to violaceous papules that occur symmetrically over the extensor aspect of the metacarpophalangeal and interphalangeal joints. Both heliotrope eruption and gottron's papules are hallmarks of dermatomyositis, not SLE. Dermatomyositis is an idiopathic inflammatory myopathy characterized by shared features of musculoskeletal weakness and muscle inflammation.
Answer D: Rheumatoid nodules are firm and painless lumps that are located on the extensor surfaces adjacent to the affected joints. Subcutaneous nodules are found in approximately 30 to 40 percent of patients with high titers of rheumatoid factor. Nodules are typically asymptomatic. Nodules occasionally develop within internal organs, achilles tendons and vocal cords. Histology includes central necrosis surrounded with palisading macrophages and lymphocytes which can test positive for rheumatoid factor. However, subcutaneous nodules are not present in the patients with SLE.
Answer E: Erythematous plaques with a silvery scale are typical of psoriasis. Psoriasis is a chronic immune-mediated skin condition. There are multiple forms of psoriasis however, plaque psoriasis is the most common form. It can be associated with nail pitting and arthritis as well. Silvery scales are not a part of the diagnostic criteria of SLE.
Bottom Line: Photosensitivity, malar rash, oral ulcers and discoid lesions are part of the diagnostic criteria of SLE.
For more information, see:
Agabegi S, Agabegi E. Step-Up To Medicine. 3rd ed. Philadelphia, PA. Lippincott: Williams & Wilkins; 2013: 243-244, 246.
Temperature 37.8ºC (100.0ºF)
Blood pressure 100/60 mmHg
Heart rate 70/min
Respiratory rate 16/min
Physical examination is remarkable for mild erythema and tenderness of the third, fourth and fifth metacarpal joints in the hands and wrists bilaterally. Small painless ulcers are noted in the mouth as well. Laboratory analysis exhibits thyroxine 6 ug/dL, erythrocyte sedimentation rate 240 mm/hr, blood urea nitrogen 25.5 mg/dL and creatinine 1.6 mg/dL with trace proteinuria. Plain film radiography of the bilateral wrists display soft tissue swelling without joint space narrowing or bone erosions.
Which of the following is likely additional manifestation of this patient's position?
A. dusty central area with an erythematous halo
B. erythematous eruption on eyelids
C. erythematous raised patches
D. firm lumps next to flexor surfaces
E. silvery white scales
Explanation:
Mucocutaneous manifestations are involved in over 80% of patients with systemic lupus erythematosus (SLE). There are four types of mucocutaneous lesions that are a part of the American College of Rheumatology diagnostic criteria of SLE. These include malar (butterfly) rash, discoid rash, photosensitivity and oral ulcers. Discoid lesions are erythematous raised patches with adherent keratosis scaling which can present on the face, neck, and scalp. Another common dermatological lesion seen in SLE is a malar rash, an erythematous rash located over the malar eminences with sparing of the nasolabial folds. These rashes are generally photosensitivity as they worsen or manifest after sun exposure.
Answer A: A target lesion contains a dusky central spot with a dark red inflammatory zone and an erythematous halo on the extreme periphery of the lesion. A target lesion is the hallmark of erythema multiforme (EM) and is not typical of SLE. EM is an acute, immune-mediated condition induced by infection, medications, malignancy and/or autoimmune disease. These lesions are accompanied by erosions involving the oral, genital and/or ocular mucosa. Nonspecific laboratory analysis include elevated erythrocyte sedimentation rate, white blood cell count, and hepatic transaminases. EM is a self-limiting disease that resolves within weeks.
Answer B: A heliotrope eruption is an erythematous eruption located on the upper eyelids with edema. Gottron's papules are erythematous to violaceous papules that occur symmetrically over the extensor aspect of the metacarpophalangeal and interphalangeal joints. Both heliotrope eruption and gottron's papules are hallmarks of dermatomyositis, not SLE. Dermatomyositis is an idiopathic inflammatory myopathy characterized by shared features of musculoskeletal weakness and muscle inflammation.
Answer D: Rheumatoid nodules are firm and painless lumps that are located on the extensor surfaces adjacent to the affected joints. Subcutaneous nodules are found in approximately 30 to 40 percent of patients with high titers of rheumatoid factor. Nodules are typically asymptomatic. Nodules occasionally develop within internal organs, achilles tendons and vocal cords. Histology includes central necrosis surrounded with palisading macrophages and lymphocytes which can test positive for rheumatoid factor. However, subcutaneous nodules are not present in the patients with SLE.
Answer E: Erythematous plaques with a silvery scale are typical of psoriasis. Psoriasis is a chronic immune-mediated skin condition. There are multiple forms of psoriasis however, plaque psoriasis is the most common form. It can be associated with nail pitting and arthritis as well. Silvery scales are not a part of the diagnostic criteria of SLE.
Bottom Line: Photosensitivity, malar rash, oral ulcers and discoid lesions are part of the diagnostic criteria of SLE.
For more information, see:
Agabegi S, Agabegi E. Step-Up To Medicine. 3rd ed. Philadelphia, PA. Lippincott: Williams & Wilkins; 2013: 243-244, 246.
Question 3: A 32-year old African American female presents with wrist pain of 12 weeks' duration. Review of system is positive for fatigue, malaise, myalgias, and morning stiffness. Past medical history is negative for any illnesses except a spontaneous miscarriage. Family history is significant for a mother with rheumatoid arthritis and Hashimoto's disease. Vital signs reveal the following:
Temperature 37.8ºC (100.0ºF)
Blood pressure 100/60 mmHg
Heart rate 70/min
Respiratory rate 16/min
Physical examination is remarkable for mild erythema and tenderness of the third, fourth and fifth metacarpal joints in the hands and wrists bilaterally. Small painless ulcers are noted in the mouth as well. Laboratory analysis exhibits thyroxine 6 ug/dL, erythrocyte sedimentation rate 240 mm/hr, blood urea nitrogen 25.5 mg/dL and creatinine 1.6 mg/dL with trace proteinuria. Plain film radiography of the bilateral wrists display soft tissue swelling without joint space narrowing or bone erosions.
Which of the following laboratory values are part of the diagnostic criteria for this patient's most likely condition?
A. anti-citrullinated peptide antibody
B. anti-Jo-1 antibody
C. anti-Ro/SSA antibody
D. anti-Scl 70 antibody
E. anti-Smith antibody
Temperature 37.8ºC (100.0ºF)
Blood pressure 100/60 mmHg
Heart rate 70/min
Respiratory rate 16/min
Physical examination is remarkable for mild erythema and tenderness of the third, fourth and fifth metacarpal joints in the hands and wrists bilaterally. Small painless ulcers are noted in the mouth as well. Laboratory analysis exhibits thyroxine 6 ug/dL, erythrocyte sedimentation rate 240 mm/hr, blood urea nitrogen 25.5 mg/dL and creatinine 1.6 mg/dL with trace proteinuria. Plain film radiography of the bilateral wrists display soft tissue swelling without joint space narrowing or bone erosions.
Which of the following laboratory values are part of the diagnostic criteria for this patient's most likely condition?
A. anti-citrullinated peptide antibody
B. anti-Jo-1 antibody
C. anti-Ro/SSA antibody
D. anti-Scl 70 antibody
E. anti-Smith antibody
Explanation:
ANA (anti-nuclear antibody), anti-dsDNA, antiphospholipid, and anti-smith antibodies are the four common antibodies noted to be positive in SLE. Anti-Smith (Anti-Sm) antibody is 55 to 100% specific for SLE. In contrast to anti-dsDNA antibody, anti-smith antibodies do not correlate with the extent of the disease. Anti-Sm remains positive in a patient whose disease is quiescent. Therefore, measurement of these antibodies are useful in patients when they are relatively asymptomatic.
Other antibodies include anti-doubled stranded deoxyribonucleic acid antibodies (Anti-dsDNA) which is 100% specific for SLE. Anti-dsDNA titers correlate with disease activity especially with active lupus nephritis. Antiphospholipid antibodies can also be seen in approximately one third of lupus patients. These antibodies cause certain blood-clotting complications such as stroke, pulmonary embolism, and miscarriage, as present in this patient. The criteria for antiphospholipid antibody in SLE include positive titers on abnormal serum level of IgG or IgM anticardiolipin antibodies, a positive test result for lupus anticoagulant and a false-positive test confirmed by Treponema palladium immobilization. Lastly, antinuclear antibody is part of the criteria to meet the diagnosis of SLE. However, it is not specific as it is also present in other autoimmune disorders such as rheumatoid arthritis, Sjogren's syndrome and scleroderma.
Answer A: Anti-citrullinated peptide antibodies are specific for the diagnosis of rheumatoid arthritis (RA). The main biological markers in patients with RA are rheumatoid factors, antibodies to citrullinated peptides, erythrocyte sedimentation rate, and C-reactive protein. These antibodies can be present prior to the appearance of RA symptoms which is important in early diagnosis and treatment of RA. However, these antibodies are not present in patients with SLE.
Answer B: Anti-Jo-1 antibody is specific in inflammatory myopathies such as polymyositis and dermatomyositis. It is the most common myositis-specific autoantibody. These antibodies are associated with severe clinical findings including up to 70% of those with pulmonary fibrosis, 53% of patients with Raynaud phenomenon and 12% of those with sclerodactyly. This patient does not report any signs of muscle weakness or myositis, therefore this would not be the most likely next step.
Answer C: Anti-Ro/SSA antibodies are frequently detected in patients with primary Sjogren's disease. Although Anti-Ro antibodies can also be seen in other disorders such as systemic lupus erythematous (SLE), systemic sclerosis, rheumatoid arthritis and primary biliary sclerosis, it is not specific for SLE. The presence of Anti-Ro/SSA antibodies increase the risk of developing neonatal SLE. This patient does not complains of dry eyes, dry mouth or extra glandular symptoms. Therefore, measurement of anti-Ro/SSA antibodies would not be indicated.
Answer D: Anti-Scl-70 antibody, or antitopoisomerase I, attacks the topoisomerase 1 antigen which is very specific for scleroderma. Scleroderma is a chronic systemic autoimmune disease marked by fibrosis and divided into two types, limited and diffuse. Limited scleroderma, or CREST syndrome, affects the hands, arm and face which has positive anti-centromere antibody. Diffuse scleroderma is characterized by organ involvement in addition to the skin and positive Anti-Scl-70 antibodies. This patient does not have symptoms suggestive of scleroderma making the utility of this assay unhelpful.
Bottom Line: Positive titers of antinuclear antibody and/or Anti-smith, Anti-dsDNA or anti-phospholipid antibodies are part of the immunological criteria in SLE.
For more information, see:
Agabegi S, Agabegi E. Step-Up To Medicine. 3rd ed. Philadelphia, PA. Lippincott: Williams & Wilkins; 2013: 243-244, 246.
No comments:
Post a Comment
Leave a comment with feedback, questions, or inquiries for Paul. He will try to respond within 1-2 weeks.