Intro to Electrocardiograms for Physician Assistants
Updated: 07/08/2016
Electrocardiocardiograms can be difficult to tackle and I know that this is a topic that I repeatedly visit, both for simple things like delineating PVCs (premature ventricular contractions) from PACs (premature atrial contractions) and denoting what defines a second degree type 1 versus a second degree type 2 heart block. But there’s so much more than just that - there’s right and left bundle branch blocks, right and left ventricular hypertrophy, ischemia, infarction, axis deviation, atrial hypertrophy, etc. While this is a very limited approach to EKGs and while there is still much to learn about them, this is a great introduction to EKGs for any student, whether you are pre-med, pre-PA, pre-NP, pre-nursing, or pre any other health profession. At the end of the review are a few helpful questions provided by TrueLearn you can use after you’ve studied the review, which offer you some insight into the type of questions and degree of exam preparation offered. I hope that you find them as useful as I have. Good luck and let me know if there are any errors or questions!
Electrocardiogram (ECG): records the electrical activity of the heart and information about the heart’s function and structure
Basic Principles
- A polarized myocyte has a negatively charged interior and positively charged outside surface = resting state
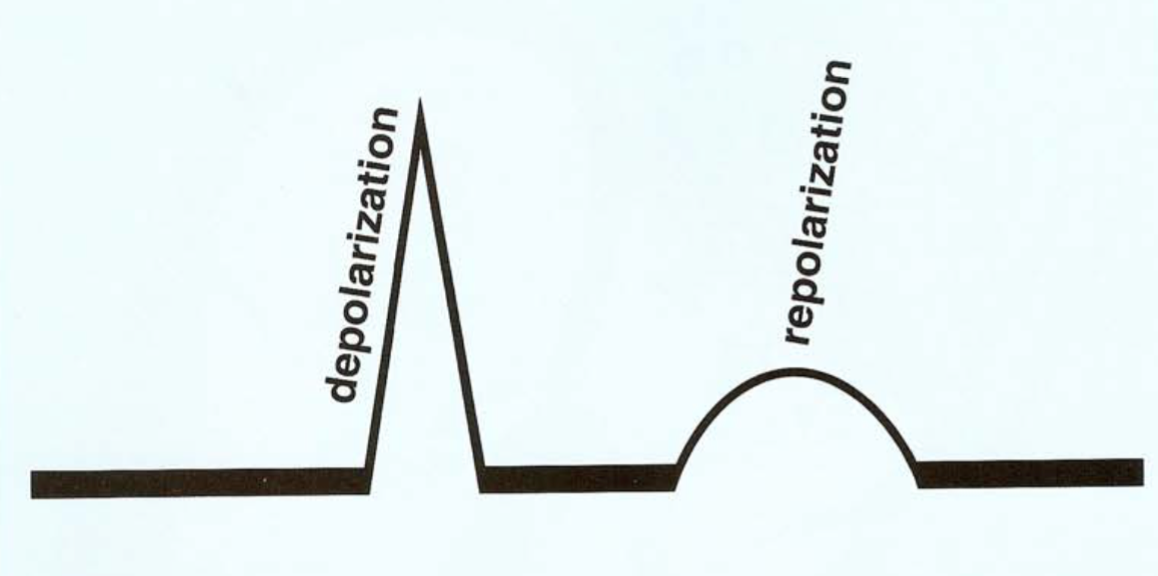
- Depolarization - occurs when myocytes interiors become positive and contraction occurs
- Repolarization - recovery phase occurring immediately after depolarization
- When a wave of positive Na+ ions moves toward a positive electrode, an upward deflection is recorded
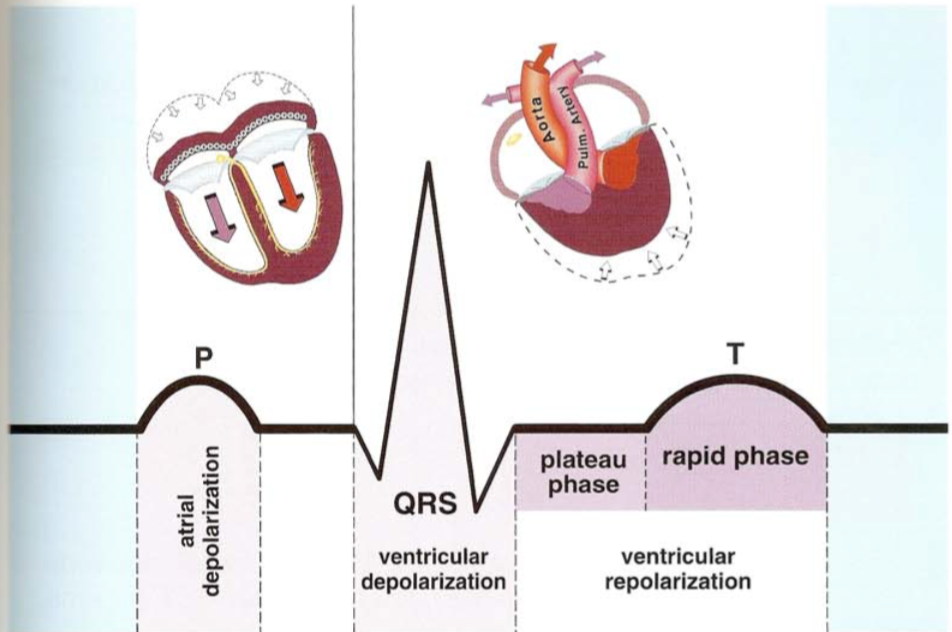
- The SA Node (upper posterior wall of right atrium) initiates depolarization at regular intervals stimulating both atria to contract and producing a P-wave (atrial depolarization)
- The tricuspid and mitral (AV) valves lie between atria and ventricles, providing electrical insulation, leaving only the AV node to conduct depolarization
- tRIcuspid on the RIght side
- AV valves also prevent backflow into the atria
- The AV Node - slow conduction by calcium ions
- Represents brief pause after P-wave before QRS complex
- Ventricular Conduction System
- QRS Wave (Purkinje Fibers): His Bundle → Left and Right Bundle Branches
- Ventricular depolarization is rapidly conducting Na+ ions, represented by the QRS complex
- Q wave: first downward deflection of the QRS complex
- R wave: first upward wave of QRS complex
- S wave: any downward wave preceded by an upward wave
- ST segment: horizontal baseline following QRS wave
- T-wave: represents the rapid phase of ventricular repolarization
- Repolarization is accomplished by potassium (K+) ions leaving monocytes
- Ventricular systole (contraction) begins with the QRS complex and lasts until the end of T wave
- QT Interval: duration of ventricular systole; measured from beginning of QRS until end of T wave → good indicator for repolarization
- Long QT Syndromes are vulnerable to dangerous (deadly) rapid ventricular rhythms
- QTc: Precise QT interval measurements are corrected for rate
- Calculated by dividing the measured QT by the square root of the R-R interval
- QTc >0.46 seconds = LQTS
- Considered normal when less than half of the R-to-R interval
- PR Interval: P wave + PR segment
- U-wave (follows T wave): repolarization of the Purkinje fibers
Physiology
- Sympathetic Nerves
- Secrete Norepinephrine that activates adrenergic receptors
- The heart is stimulated by the sympathetic NS that deliver NE to the B1 adrenergic receptors, producing an excitatory response
- Cardiac excitatory effects: increased rate of SA Node pacing, rate of conduction, contractility, and irritability of foci
- Epinephrine is secreted by the adrenal glands and is more potent than NE in stimulating B1 receptors
- Stimulation of arterial A1 adrenergic receptors constricts arteries throughout the body increasing blood pressure and flow (more responsive to NE)
- Parasympathetic Nerves
- Secrete Acetylcholine (ACh) that activates cholinergic receptors
- Cardiac inhibitory effects: decreased rate of SA node pacing, rate of conduction, contractility, irritability of atrial and junctional foci
- Arterial cholinergic receptors respond by dilating arteries and reduce blood pressure and flow
- The cardiac cycle represents atrial systole (contraction), followed by ventricular systole (contraction) and resting stage that follows until another cycle begins
- Atrial depolarization represented by the P wave
- Actually lasts longer than the P wave
- QRS complex represents ventricular depolarization
- Actually lasts longer than the QRS complex
- The release of free calcium ions into the interior of the myocytes produces contraction
- Repolarization is due to controlled outflow of K+ ions from myocytes
- Cell to cell conduction through the myocardium is carried by Na+ ions, however, AV nodal conduction is due to slow movement of calcium ions
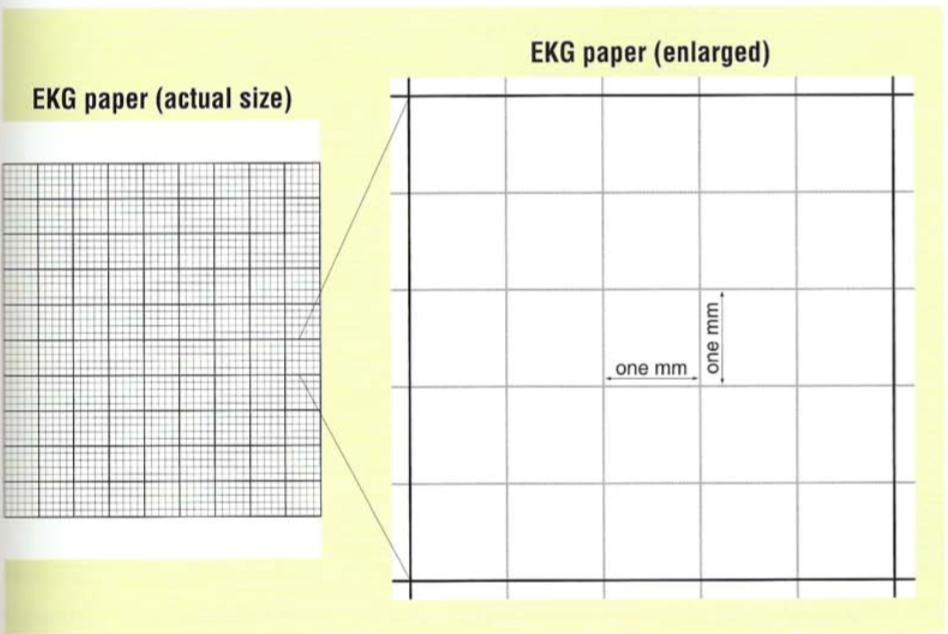
ECG Recordings
- Small boxes are 1 mm by 1 mm; each small box represents 0.04 seconds and large boxes of 5 small boxes represents 0.2 seconds
- Heavy black lines are separated by 5 small squares
- Time axis is horizontal and the vertical axis represents voltage
- Upward deflections are positive, downward deflections are negative
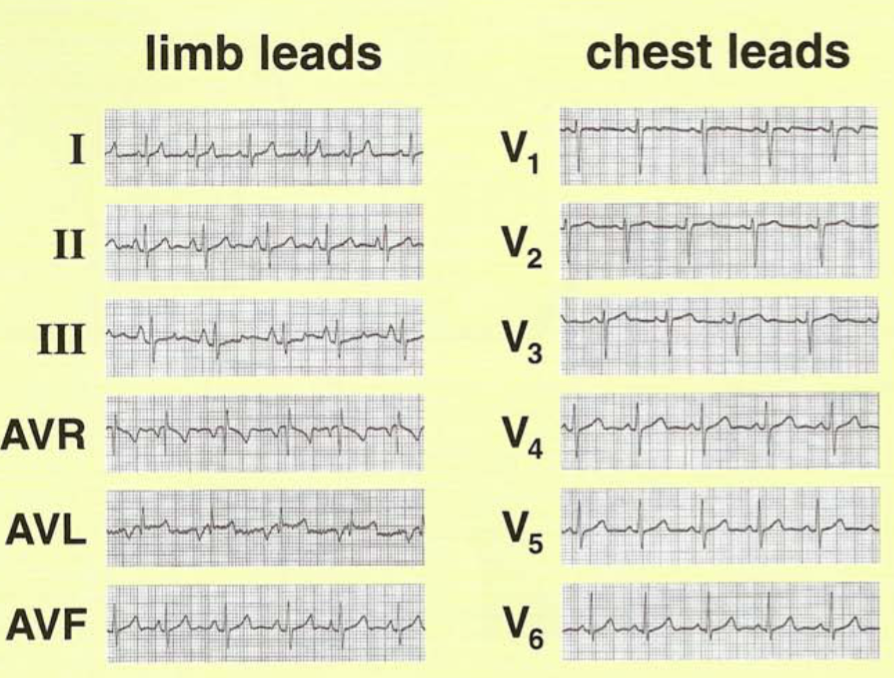
The Standard 12-Lead ECG
- Electrodes are placed on the R arm, L arm, and L leg
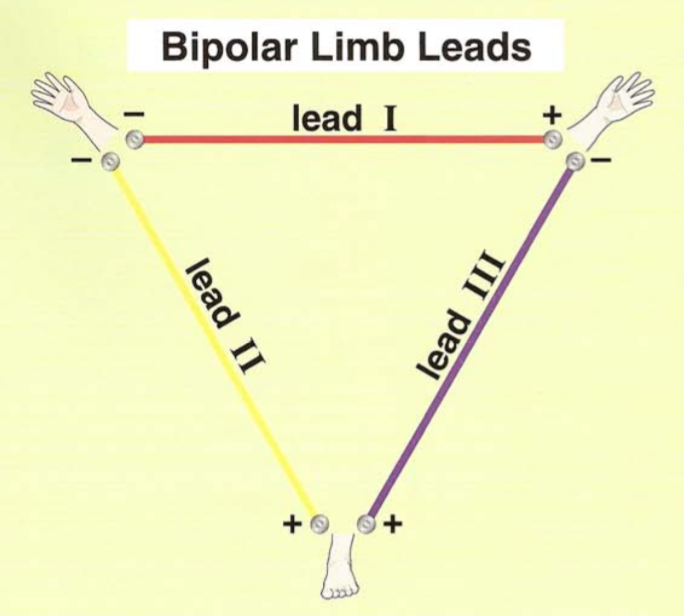
Einthoven’s Triangle
- Leads I, II, and II: Each bipolar limb lead is recorded using 2 electrodes, one being positive and the other negative
- RAN = right arm negative, LLP = left leg positive, and you can always figure out the left arm from there
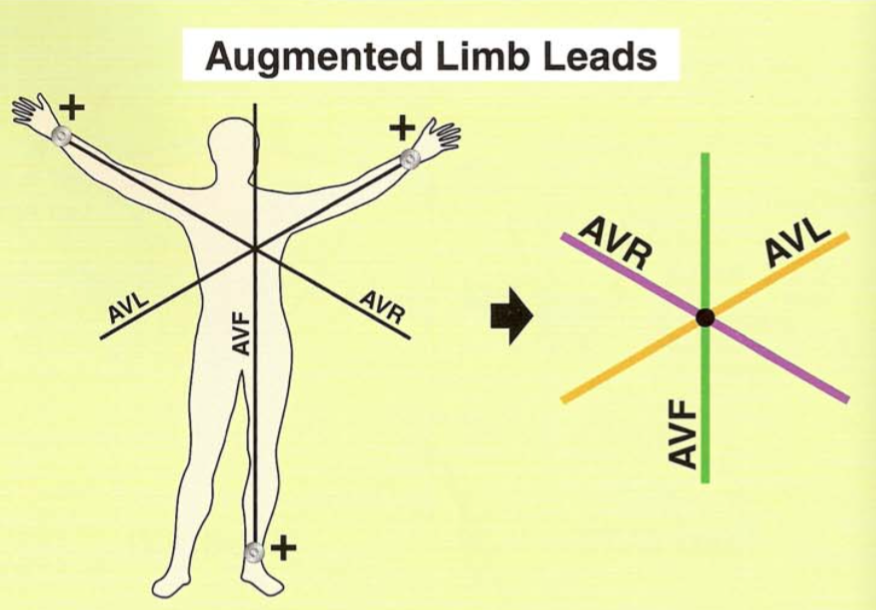
- Unipolar Limb Leads: AVF signifies the left leg electrode, which is termed AVF (Augmented Voltage, left Foot) by Dr. Goldberger who discovered that we must amplify the voltage in the machine to match the magnitude of each of the leads
- AVR (right arm), AVL (left arm), AVF (left foot) - all positive
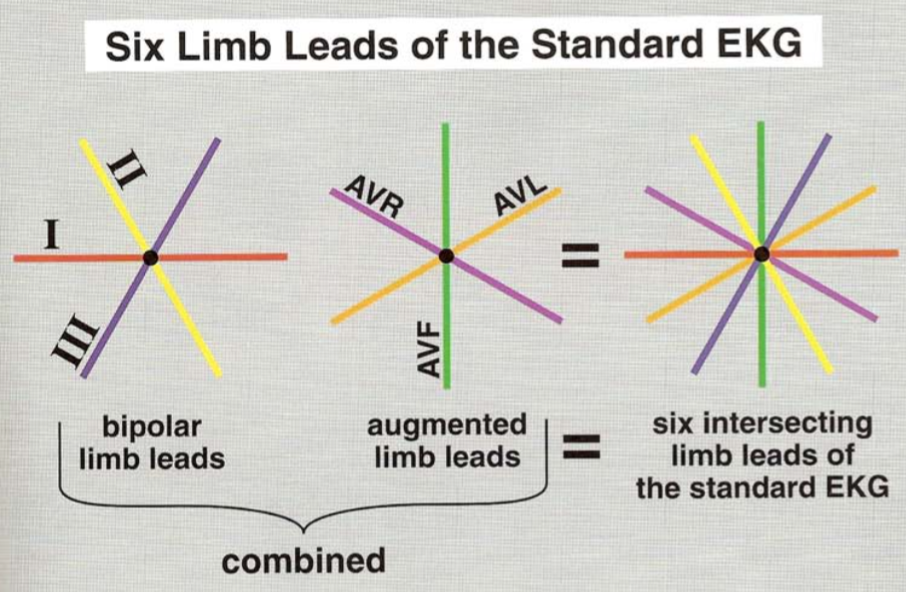
- All six limb leads form an intersection that lie in a flat frontal plane of the patient’s chest
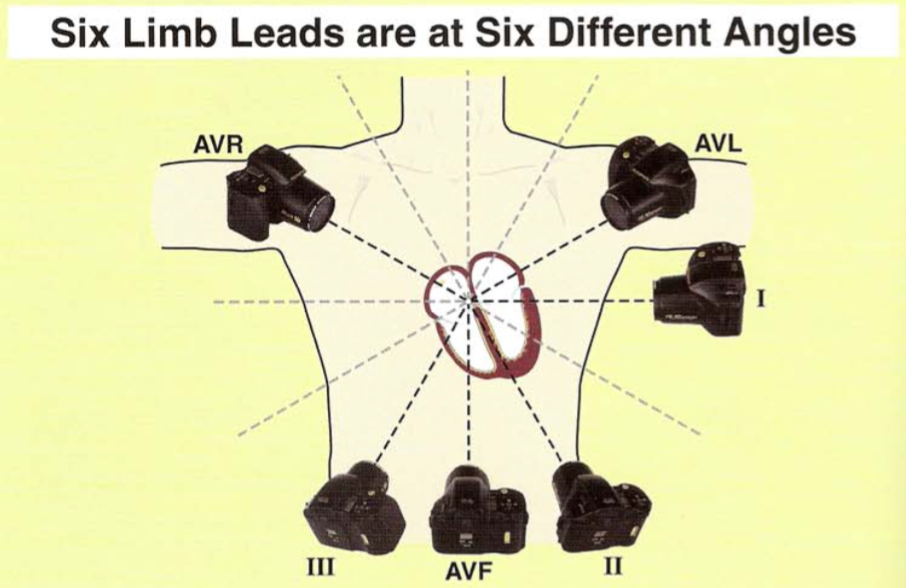
- The importance of the positive electrode’s position is emphasized by the conventional grouping of limb leads
- The ‘lateral leads’ refers to lead I and AVL (positive left arm electrode), which is important for recognizing lateral wall ischemia/infarction
- The ‘inferior leads’ refers to leads II, III, and AVF (positive left foot electrode), which is important for recognizing inferior wall ischemia/infarction
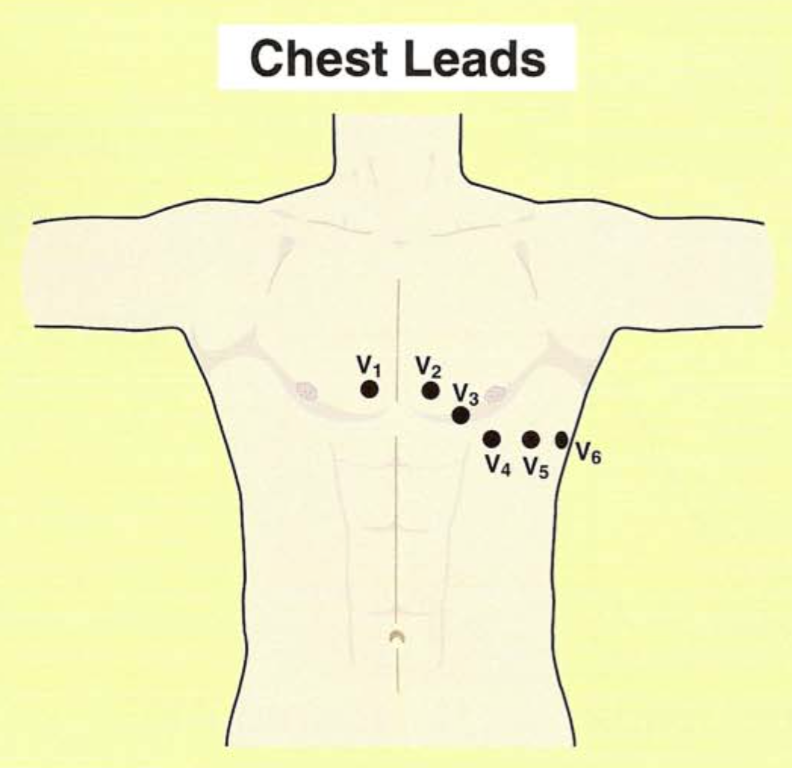
- The chest leads (V1-V6) are oriented through the AV node and projections anterior to posteriorly through the patient’s back, which is negative
- The plane is called the horizontal plane
- V1 and V2 cover the right ventricle, signify the anterior wall
- V5 and V6 cover the left ventricle and signify the lateral wall
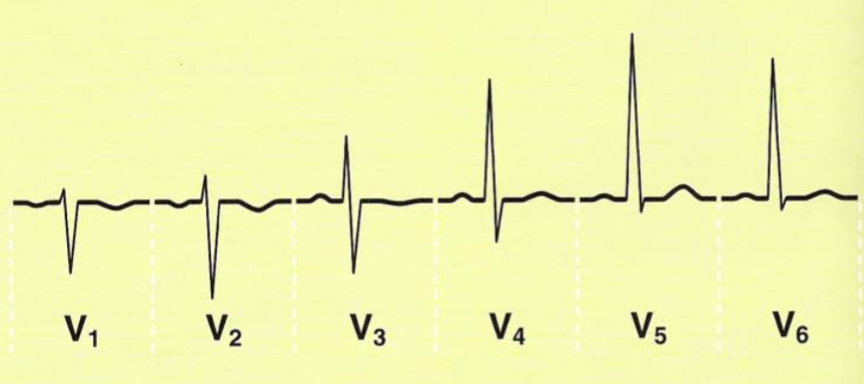
- Leads V1-V6 should gradually change
- V1’s QRS complex is normally more negative
- V6’s QRS complex is normally more positive
- V3 and V4 are oriented over the interventricular septum (right and left bundle branches course through)
- V5 and V6 are called the left chest leads and are positive because of their position around the heart; greater upward deflections are caused by depolarization moving toward the positive electrode
Terminology
- Automaticity: the generation of pacemaking stimuli
- Automaticity (ectopic) foci: focal areas of automaticity in the heart that are potential pacemakers capable of pacing in emergency situations; normally electrically ‘silent’
- These have the ability to pace at their inherent rate if SA node ceases to function
- Atria: 60-80/minute
- AV Junction: 40-60/minute
- Ventricles: 20-40/minute
- SA node overdrive-suppresses slower pacemaker foci below it
- All automaticity foci pace with a regular rhythm
- Vagal Maneuvers: induced gagging or carotid sinus massage provide afferent input for parasympathetic reflexes that counterbalance sympathetic effects → can inhibit an irritable atrial or AV junctional focus or inhibit AV node completely increasing refractoriness
- Arrhythmia (Dysrhythmia): without rhythm; denotes any abnormal rhythm
- Absolute Refractory Period: no impulse possible
- Relative Refractory Period: Impulse possible if stimulus strong enough
- Parasystolic focus: an automaticity focus that has entrance block meaning the focus paces, but cannot be overdrive-suppressed; incoming depolarization is blocked, ‘protecting’ foci from passive depolarization by other sources (not healthy)
- P’ (P prime): represents atrial depolarization by an automaticity focus, as opposed to normal sinus-paced P waves
- Asystole: all activity ceases (straight line), no electrical activity
- Pulseless electrical activity (PEA): rhythm on the monitor but no pulse
- Unifocal: single ventricular focus in which all ectopic beats appear identical
- Multifocal: several ventricular foci that have multiple configurations
- Runs: 3+ premature ventricular contractions occurring in succession
- Couplets: 2 PVCs attach to one another
- Bigeminy: PVCs falling in a pattern of ‘every other beat’
- Trigeminy: repetitive PVC followed by 2 sinus beats (3 beats)
- Quadrigeminy: pattern of 4 beats (1 PVC and 3 sinus beats)
- Heart blocks: caused when a supraventricular impulse is unable to be conducted normally through the ventricles because of a conduction disturbance at or below the AV node
- Bundle Branch Blocks: caused by a conduction defect below the area of the node, within the branches of the ventricular conduction system
- Non conducted P waves: “blocked” p waves or “dropped” QRS complexes
- Agonal: dying heart, describes a terminal or lethal arrhythmia
- Escape beat: comes later than expected and is a fail-safe to protect the heart
Method to Interpreting an ECG
- Rate: number of cycles per minute
- Sinus rhythm determined by SA node (pacemaker), normally 60-100
- Sinus bradycardia: sinus rhythm <60/minute
- Sinus tachycardia: sinus rhythm >100/minute
- Determining the rate
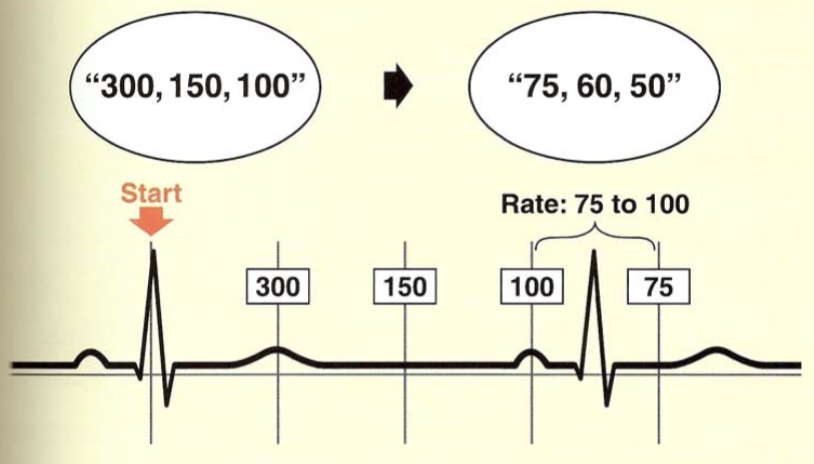
- The ‘300’ Method: Find an R wave that peaks on a heavy black line (start)
- Works for regular intervals
- Count off 300, 150, 100, 75, 60, 50 at each subsequent line (memorize this)
- So a normal rate = R-R should be between 3-5 lines from one another
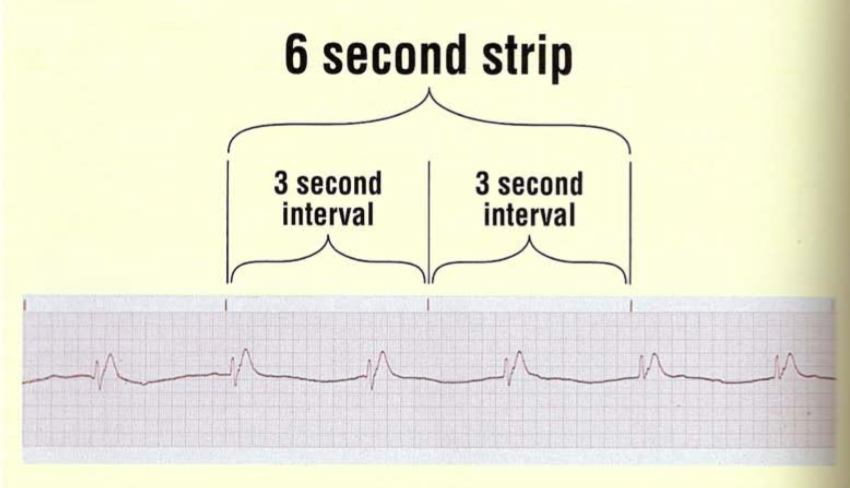
- For bradycardias and irregular rhythms: Use The ‘3 Second’ Intervals Method
- Identify the ‘3 second’ marks
- Take 2 of the 3-second intervals and count the number of R-R wave cycles per 6 seconds
- Multiply by 10 to get the number per minute
- Rhythm
- SA Node automaticity maintains a constant cycle duration between impulses, maintaining a regular rhythm
- Irregularity: pauses, presence of too-early (premature) beats, sudden dramatic rate changes
Sinus Rhythms
Sinus Bradycardia
|
Rate: Slow <60
Rhythm: Regular
P-wave: normal
PR interval: Normal (0.12-0.20 s)
QRS: Normal (0.06-0.10 s)
|  | |
Sinus Arrhythmia
Normal, but minimal, increase in heart rate during inspiration and extremely minimal decrease during expiration
|
Rate: Normal (60-100) and may increase with inspiration and decrease with expiration
Rhythm: Irregular (R-R varies without pattern)
P-wave: Uniform, one P wave for every QRS complex
PR interval: Normal (0.12-0.20 s)
QRS: Normal (0.06-0.10 s)
|  | |
Sinus Tachycardia
Ex. hypotension, hypoxia, CHF, cardiomyopathy, myocarditis, anemia, fever, bleeding
|
Rate: Fast (>100)
Rhythm: Regular
P-wave: normal, may merge with T wave at very fast rates
PR interval: Normal (0.12-0.20 s)
QRS: Normal (0.06-0.10 s)
QT interval shortens with increasing rate
|  | |
Irregular Rhythms
Wandering Pacemaker
|
Rate: Normal
Rhythm: May be irregular
P-wave: changing shape and size from beat to beat (>3 forms)
PR interval: variable
QRS: Normal (0.06-0.10 s)
T wave normal, if heart rate >100, rhythm may be MAT
|  | |
Multifocal Atrial Tachycardia (MAT)
Ex. COPD, emphysema, digitalis toxicity
|
Rate: Fast >100
Rhythm: irregular
P-wave: changing shape and size from beat to beat (>3 forms)
PR interval: variable
QRS: normal (0.06-0.10 s)
|  | |
Premature Atrial Complex (PAC)
Ex. Stress, hypoxia, stimulants (caffeine, tobacco, alcohol), valvular heart disease, CAD
|
Rate: Normal
Rhythm: irregular
P-wave: premature, positive, shape is abnormal; flattened, notched, peaked or diphasic; falls close to preceding QRS
PR interval: variable
QRS: 0.10 s or less (narrow)
|
Asymptomatic or palpitations
Observation
Beta blockers if SX
| |
Junctional Tachycardia
Originates in the Bundle of His, 3 or more PJC’s in a row
|
Rate:
Atrial rate: 100-180
Rhythm: Regular
P-wave: superimposed on T waves
PR interval: none
QRS: Narrow (<0.10 s)
|  | |
Atrial Tachycardia
Ex. Stress, hypoxia, stimulants (caffeine, tobacco, alcohol), COPD, valvular heart disease or CAD, ASD, or AMI
Arises from a focus in the atria
|
Presents as palpitations, light-headedness, and/or syncope
Rate: 150-250, atrial = ventricular
Rhythm: regular
P-wave: premature, positive, shape is abnormal (but present in front of each QRS)
PR interval: variable (0.12-0.20 s)
QRS: Normal
| 
Transient, usually requires no treatment
| |
Paroxysmal Supraventricular Tachycardia, PSVT
Originates above the ventricles
|
A descriptive term for indistinguishable Junctional tachycardia, atrial tachycardia, atrial flutter, and sinus tachycardia
Atrial rate: 150-250, may conduct to ventricles 1:1, 2:1, 3:1, or 4:1 in presence of block
Ventricular rate: 150-250
Rhythm: irregular
P-wave: premature, positive, shape is abnormal; may be absent
PR interval: variable (<0.12 s)
QRS: Normal (<0.12 s)
Complication of Wolff-Parkinson-White Syndrome
| 
Stable -
a. Vagal Maneuvers: Valsalva maneuver, bearing down, cough, breath holding, carotid sinus massage
b. Med - Adenosine IV 6 mg push, flush, 12 mg in 2 minutes (slows AV conduction and interrupts reentrant pathways)
Prevention -
a. Digoxin
b. Radiofrequency catheter ablation
| |
Atrial Flutter
MCC: heart failure
Also, COPD, rheumatic fever, or ASD
AV node cannot conduct all impulses
|
Presents as palpitations, SOB, near syncope or syncope, CVA/TIA
Rate: Fast (250-350 atrial), slower ventricular rate (150-250)
Rhythm: Regular or irregular
P-wave: Non observable, saw-toothed flutter waves
PR interval: unmeasured
QRS: Normal (0.06-0.10)
| 
Stable -
a. Rate control: BB or CCB Esmolol, Verapamil, Diltiazem
b. Cardioversion 50 J
C. Anticoagulants and rate control prior
| |
Atrial Fibrillation (irregularly irregular)
Continuous chaotic atrial spikes from multiple irritable atrial foci, suffering from entrance block, pacing rapidly
At high risk for VTE and hemodynamic compromise if underlying heart disease
Most common causes: hyperthyroidism and mitral stenosis
|
Rate: Fast (>350 atrial, chaotic), slower ventricular rate
Rhythm: irregularly irregular
P-wave: No discernable p-waves
PR interval: unmeasured
QRS: <0.12 s (narrow)
|
Presents with fatigue, exertional dyspnea

1.If Stable -
a. Rate control: 60-100, Beta blockers preferred
-Non dihydropyridine CCB
b. Cardioversion to sinus rhythm (first A-fib, worsening, or hemo-unstable)
c. Anticoagulation to prevent CVA
-If present >48 h, anticoag with Warfarin for 3 weeks before and 4 weeks after cardioversion, INR 2-3
-May obtain TEE → IV heparin and cardioversion within 24 h
2. Unstable (decompensated HF, hypotension, uncontrolled angina): Cardioversion 200 J
3. Chronic A-Fib
-Rate control: BB
-Anticoagulation: not for young (<60)
4. New Onset - rate control
-CCB or BB: Diltiazem or Metoprolol
-Anticoag: IV Hep or LMWH
| |
Ventricular Rhythms
Premature Ventricular Complex (PVC)
Single ectopic beat originating in the ventricles
Benign
Occur with ischemia or electrolyte disturbances
Occurs in patients with or without structural heart disease: hypoxia, electrolyte imbalance, stimulants, caffeine, meds, heart disease
|
Wide, bizarre QRS complexes followed by compensatory pause → p wave unseen because “buried” within QRS complex
Rate: Depends on underlying rhythm and number of ectopics
Rhythm: Regular
P wave: None, buried within QRS, compensatory pause
PR interval:
QRS: >0.12 (wide)
|
Asymptomatic or palpitations
If low CO → syncope, dizziness, sudden death
1. Observation!
2. BB or CCB if symptomatic, otherwise untreated
Patients with FREQUENT, REPETITIVE PVCs and underlying cardiac disease - increased risk for sudden death due with V. Fib → electrophysiologic study
|
Ventricular Tachycardia: originates below bundle of His
“Wide QRS tachycardia”
HX of MI (Scar), ischemic CAD, QT prolongation, hypoxia, electrolyte imbalance, drug toxicity, CM
|
V-tach: 3+ consecutive ventricular premature beats
Rate: 100-250 bpm
Rhythm: Regular or irregular
P wave: none preceding QRS
PR interval: none
QRS: >0.12 (wide), bizarre but uniform
Sustained: persists in absence of intervention, lasts longer than 30 seconds, almost always symptomatic
-Hypotension, life-threatening → V-fib
|
SX: palpitations, dyspnea, lightheadedness, angina, syncope or near-syncope
-Sudden cardiac death
-Cardiogenic shock
-”Cannon A” waves in neck and S1 varying in intensity
Does not respond to vagal maneuvers or adenosine
1. Treat reversible causes
Sustained VT -
ACLS, shock, antiarrhythmics, CPR
a. Stable = IV amiodarone
b. Unstable = synchronous DC Cardioversion → IV amiodarone or Lidocaine
c. Eventual ICD placement
Non-sustained VT - brief, self-limited, asymptomatic
If CAD/LV dysfunction → risk factor for sudden death
a. No heart disease or asymptomatic → no treatment
b. Heart disease, recent MI, LVD → electrophysiology study
Post-MI: poor prognosis
|
Ventricular Fibrillation
|
Rate: cannot be determined
Rhythm: chaotic, irregular
P wave: none
PR interval: indiscernible
QRS: none
No T waves
|
Sudden unconsciousness and death, early morning
Cannot measure BP; absent heart sounds and pulse
1. Severe hypotension or LOC → synchronized cardioversion
2. Pulseless v-tach: immediate defibrillation and CPR
-If continued → 1 mg IV bolus epinephrine, then q 3-5 minutes
-Defibrillate q 30-60 seconds
-Refractory Vfib: IV amiodarone, followed by shock
If cardioversion successful: continuous IV infusion of effective drug, implantable ICD
|
Junctional Rhythms - not covered
Heart Blocks
- A prolonged PR interval is >0.2 seconds (5 small boxes, or one large square)
First Degree
Obstruction at AV node incomplete; all impulses conducted but delayed
Causes: inferior MI, drug effect
|
Rate: varies
Rhythm: Regular (NSR, brady, or tachy)
P-wave: upright, uniform, one p-wave for each QRS complex
PR interval: prolonged, but all same length (>0.20 s)
QRS: <0.12 s
|
Usually asymptomatic, patient typically an athlete
No treatment
|
Second Degree Type I (Wenckebach)
Site within AV node
Causes: vagal stimulation, ischemic heart disease, acute inferior wall MI
Drugs: BB, CCB, digitalis
|
Rate: varies
A: 60-100
V: <100, varies (faster than type II)
Rhythm: Irregular ‘grouped beating’
P-wave: normal shape and size, not every wave followed by QRS
PR interval: gets progressively longer until dropped QRS complex
QRS: <0.12 s
P:QRS ratio 3:2, 4:3, 5:4
|
Usually asymptomatic with irregular pulse w/ dropped beats
|
Second Degree Type II (Mobitz)
Site of block within His-purkinje system
Etiology: acute anterior wall MI, calcific aortic stenosis
|
Rate: varies
Rhythm: Regular or irregular
A: 60-100 (2-4 x ventricular)
V: <60, bradycardia
P-wave: Normal, more than 1 wave for each QRS
PR interval: constant, may be prolonged (usually normal)
QRS: <0.12 s
P:QRS ratio of 3:1, 4:1, 5:1
|
Presents with irregular pulse and occasional dropped beats, LOC

1. Shock if symptomatic
-Vagal maneuvers produce a 2:1 AV block → 1:1 AV block (eliminate or no effect)
2. Temporary transthoracic or transvenous pacing → permanent pacing
3. If asymptomatic, Atropine 0.5 mg IV
-If on BB, discontinue
|
Third Degree (Complete Heart Block)
All P-waves blocked at AV node, ventricles won’t contract unless another failsafe mechanism kicks in
Due to lesion distal to His bundle
Etiology: CV surgery, congenital, trauma, CM, aortic stenosis, acute inferior wall MI, Lyme disease
|
Rate: varies (25-40)
Rhythm: Regular (NSR, brady, or tachy)
P-wave: normal
PR interval: inconsistent
QRS: >0.12 s (WIDE)
|
Presents with dizziness, palpitations, syncopal attacks, angina, CHF (SOB)
1. Temporary transthoracic or transvenous pacing → permanent pacing
2. Atropine 0.5 mg IV
3. Epinephrine IV drip 2-20 mcg/min OR Dopamine 2-10 mcg/min
|
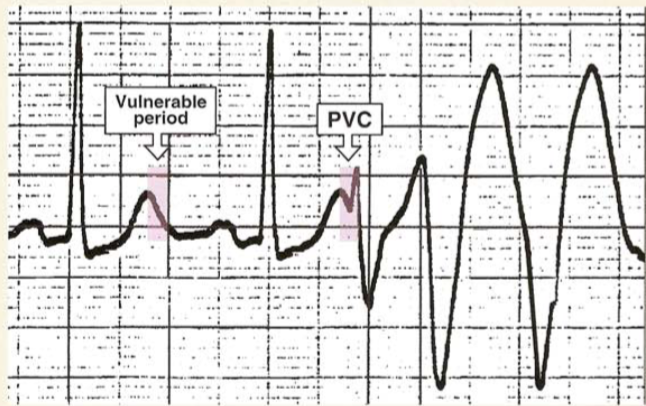
R on T Phenomenon
Precursors for ventricular tachycardia or fibrillation, Torsades, and sudden death
Cause: hypoxia or hypokalemia
|
R wave falls on or near the T wave of preceding beat, representing a ventricular depolarization of an ectopic beat on preceding T wave
|  |
QT Prolongation (Long QT Syndrome)
Precursor to lethal arrhythmia with structurally normal heart
Ex. acquired (electrolytes, antibiotics, psych meds, ischemia), congenital
Electrolyte: hypokalemia, hypomagnesemia, hypocalcemia, Hypothyroidism
FQ and macrolides (Clarithromycin, Azithromycin)
SNRI, SSRI
All antipsychotics, TCAs and antifungals (fluconazole)
Adderall (Ritalin) for people with congenital long QT
Ranolazine, Quinidine
Lidocaine, Mexiletine
Dofetilide, Amiodarone, Sotalol
Propranolol
|
Presents with palpitations, Recurrent syncope, death
Pathologic prolongation of QT interval, less than 50% R-R
Normal QT varies with heart rate
0.39 male
0.41 female
| 
Treat electrolyte abnormalities and D/C drugs that prolong QT
|
Torsades de Pointes (“Twisting of Lights”): rapid polymorphic V-tach
DANGEROUS: can lead to V-fib
Factors that prolong QT: congenital, TCAs, anticholinergics, electrolyte abnormalities, ischemia
|
Gradual change in amplitude and twisting of QRS around isoelectric line
Hypokalemia
Hypomagnesemia
|
Occurs spontaneously
IV magnesium, correct electrolyte abnormality
Remove offending drugs
Isoproterenol infusion and overdrive pacing after initial therapy
Recurrent - permanent pacemaker
|
Wolff-Parkinson-White Syndrome
A narrow complex SVT, accessory AV conduction pathway originating in the bundle of Kent
|
Rate: Tachycardia
Rhythm: Regular
P-wave: before each QRS, identical
PR Interval: <0.12 (short), decreased
QRS: >0.10 (wide)
2. Delta waves
|
1. Chest pain
-Sudden onset
-Without exertion
-Lasts 10-20 mins
-Can describe as chest heaviness
-Resolves spontaneously
-Recurrent episodes
2. Palpitations and SOB
3. Lightheadedness, chest pain lasting longer
4. Syncope
Tachycardic, hypertensive, cool, diaphoretic
Terminating acute episodes
-Vagal maneuvers
-AV blockade: IV adenosine 6-12 mg
1. Radiofrequency catheter ablation (preferred)
2. Adenosine 6 mg IV push, flush, 12 mg in 2 minutes: Antiarrhythmics to slow accessory conduction
3. AV node blocking drugs
-Avoid in acute setting
Avoid: CCB (Verapamil), Digoxin → both increase ventricular rates
|
Sinus Sick Syndrome
Abnormality of cardiac impulse formation that may be caused by an intrinsic disease of sinus node that makes it unable to pace-make or by extrinsic causes
MC: elderly patients with heart disease
May occur in heart surgery patients
Caused by scarring of heart’s conduction system
Worse with: digitalis, CCB, BB, sympatholytic agents, anti-arrhythmic drugs, aerosol propellant abuse
|
1. Sinus bradycardia, sinus arrest, sinoatrial block, alternating patterns of bradycardia and tachycardia, 2. Loss of P waves
|
1. Most asymptomatic
2. Non-specific: fatigue, irritability, memory loss, lightheadedness, palpitations
3. Syncope, presyncope, palpitations, dizziness, confusion, HF, palpitations, decreased exercise tolerance
1. Symptomatic - atrial or dual-chamber permanent pacemaker
-Provides effective relief of symptoms
-Lowers incidence of atrial fibrillation, thromboembolic events, heart failure, and mortality
-Digitalis can cause bradyarrhythmias in SSS
Complications: myocardial perforation, pneumothorax, wound hematoma, venous thrombosis, pacemaker lead failure, infection
|
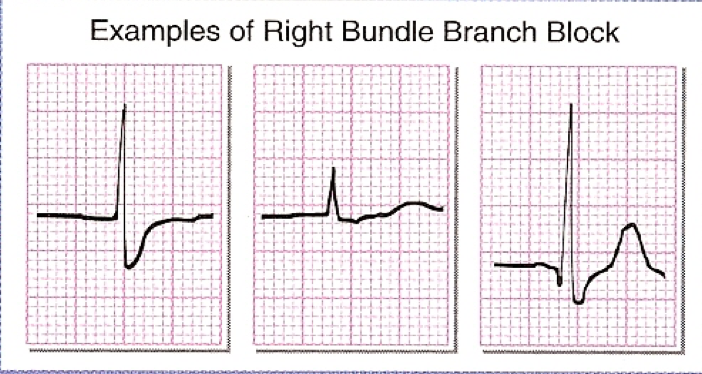
Bundle Branch Blocks
Right Bundle Branch Block
|
Left Bundle Branch Block (Deep S)
| |
V1
|
 |
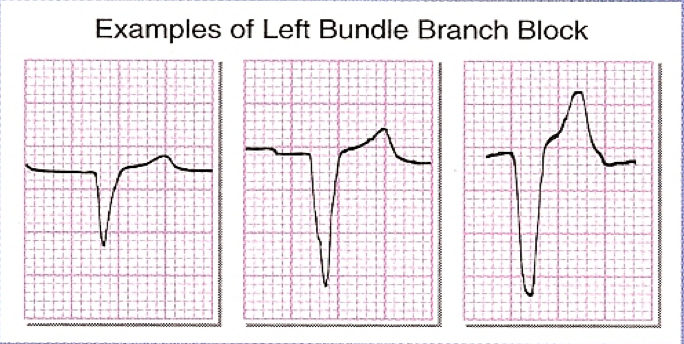 |
V6
|
 |
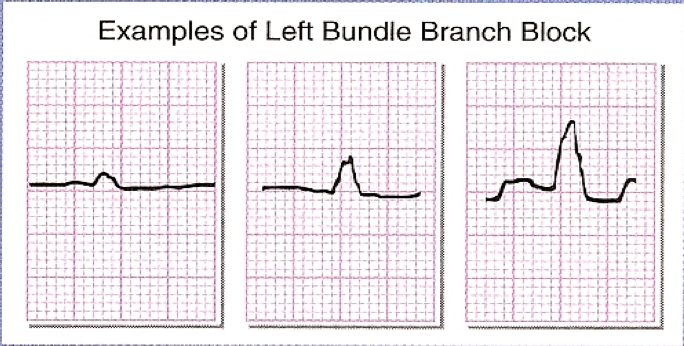 |
- A ST pattern of LBBB may obscure or mimic ST changes associated with ischemia or infarct
Sgarbossa’s Criteria for Acute Injury with LBBB
- (1) Discordance is good, unless excessive (>5 mm) = 2 points (least predictive)
- Appropriate discordance is expected → suspect acute injury
- (2) ST depression (>1 mm) is concordant in V1-V3 = 3 points → suspect acute injury
- (3) ST elevation (>1 mm) is concordant = 5 points → suspect acute injury
- Axis
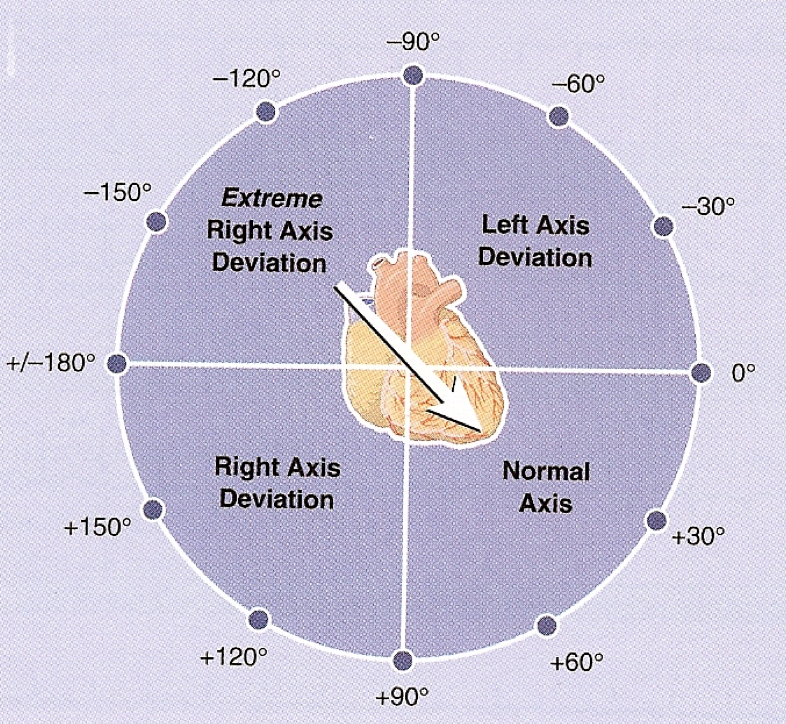
- The Quadrant Method (most efficient)
- Look at Leads I and aVF and identify the quadrant the axis is in based on the table below
- The Isoelectric Lead (most precise)
- Identify the limb lead that is most isoelectric (equal upward and downward deflection)
- Identify the vector 90 degrees perpendicular to the isoelectric lead → calculate the QRS axis
Lead I
|
Lead AvF
| |
Normal (0 to +90)
|
Upward
|
Upward
|
Right Axis Deviation (+90 to 180)
|
Downward
|
Upward
|
Extreme Right Axis Deviation (180 to -90)
|
Downward
|
Downward
|
Left Axis Deviation (-90 to 0)
|
Upward
|
Downward
|
- Hypertrophy (Enlargement)
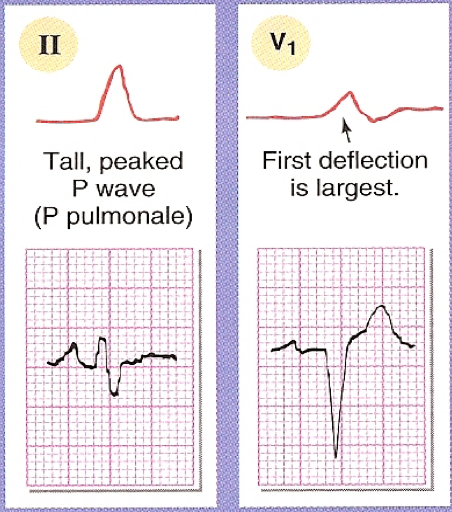
Atrial Hypertrophy
Lead
|
Right Atrial Enlargement
Look at first half of P wave
|
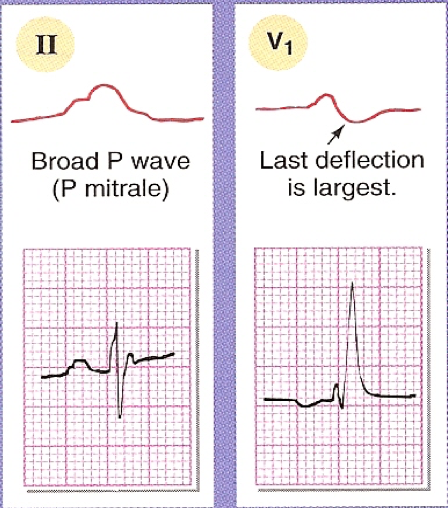
Left Atrial Enlargement
Look at second half of P wave
|
II
|
Tall, peaked P wave (P pulmonale)
|
Broad P wave (P mitrale)
|
V1
|
First deflection is largest
|
Last deflection is largest
|
 |  |
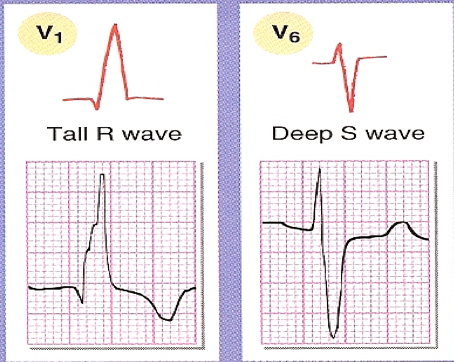
Ventricular Hypertrophy
Lead
|
Right Ventricular Enlargement
|
Left Ventricular Enlargement
|
V1
|
Tall R wave
|
Deep S wave
|
V6
|
Deep S wave
|
Tall R wave
|
 | 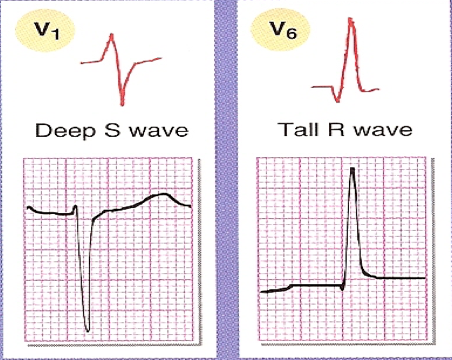 |
Rule of 35: verifies presence of left ventricular enlargement (LVH)
- Measure depth of deepest wave in V1 or V2
- Add height of tallest wave in V5 or V6
- If sum is >35 mm and patient >35, criteria for LVE met
- Largest R and Largest S > 45 mm in any precordial leads (V1-V6)
- R wave in AvL > 11 mm
- R wave in AvF > 20 mm
- R wave in I and S wave in III > 25 mm
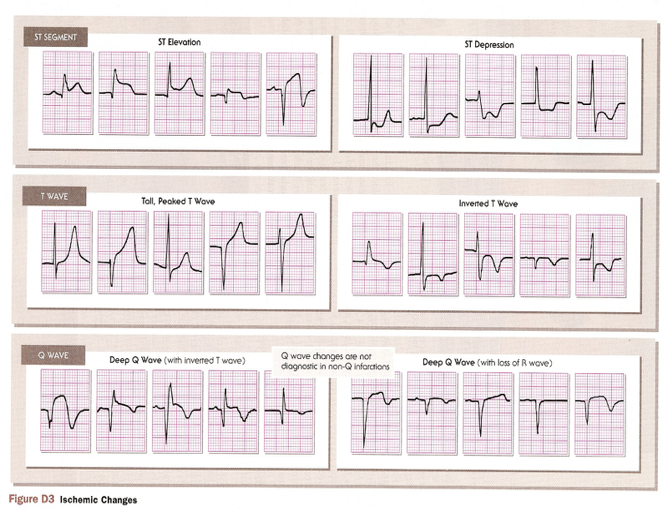
- Infarction and Ischemia
Coronary Arteries of the Heart
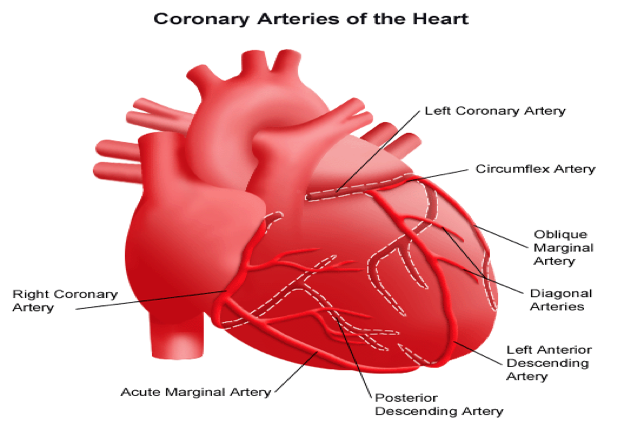
- RIP: RCA (right coronary artery) = Inferior + Posterior
- LAL: LCA (left coronary artery) = Anterior + Lateral
Inferior Wall
|
II, III, AvF
|
Lateral Wall
|
I, AvL, V5-V6
|
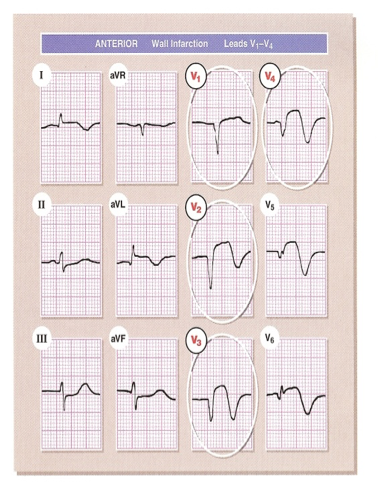
Anterior Wall and Septum
|
V1-V4
|
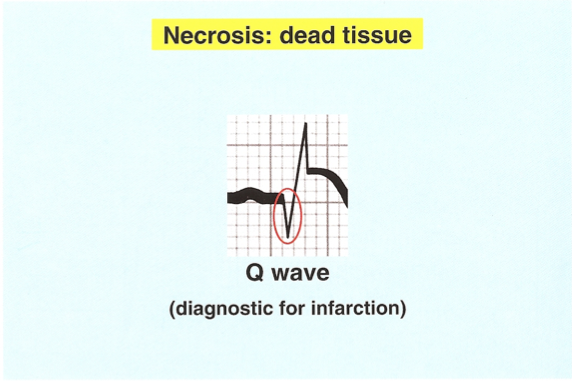
Acute Injury
|
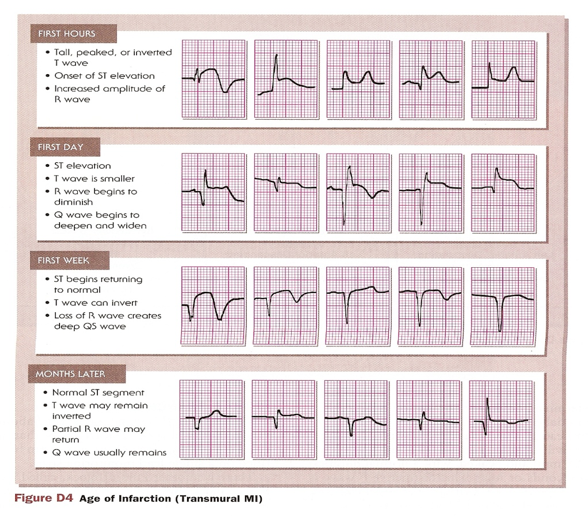
Old Infarction (Q waves)
|
 |  |
- Always give priority to ST elevation, if present
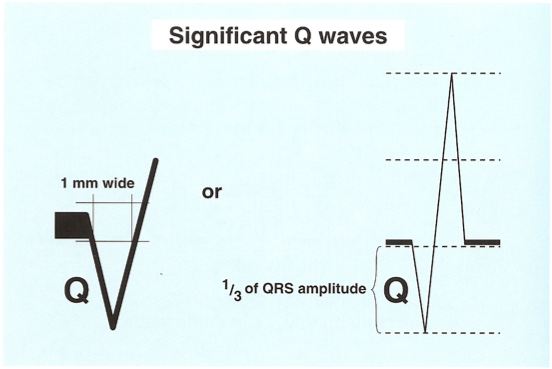
Significant Q Waves
- 1 mm wide (1 small box) or ⅓ QRS amplitude
Acute Injury
Anterior Wall Infarction
Leads: V1, V2, V3, V4
|  | |
Inferior Wall Infarction
Leads: II, III, aVF
|  | |
Lateral Wall Infarction
Leads: I, aVL, V5, V6
|  | |
Posterior Wall Infarction
|
Acute Posterior Infarction = ‘ST Depression’
|
 |  |
- Posterior Wall MI: ST depression rather than elevation, upright T-wave, and tall, broad R wave (Q wave seen in reverse)
6. Other Findings
COPD
|  |
1. Multifocal Atrial Tachycardia
2. Small amplitude in EKG leads
3. Right axis deviation
|
Pulmonary Embolus
| 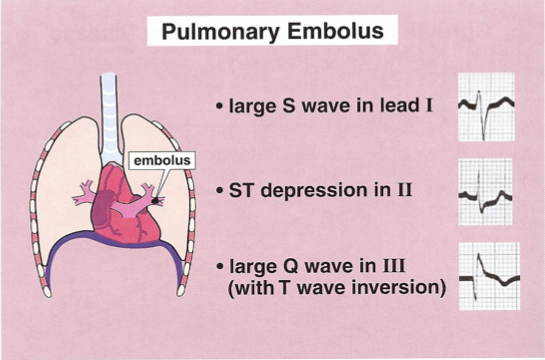 |
S1 Q3 T3
Lead I: large S wave
Lead II: ST depression
Lead III: Large Q wave in III with T wave inversion
V1-V4: T wave inversion
Transient RBBB
|
Hyperkalemia
|
Hypokalemia
|
|
|
Hypercalcemia
|
Hypocalcemia
|
|
|
Cardioversion vs. Defibrillation
Indications
| ||
Cardiac Pacemakers
|
- Delivers direct electrical stimulation to heart when heart’s natural pacemaker is unable to do so
|
-Sinus node dysfunction, also known as sinus sick syndrome (MC): with symptomatic bradycardia, HR <40 bpm, minimal symptoms with HR <30,
-Symptomatic heart block (mobitz type II and complete)
-Symptomatic bradyarrhythmias
-Tachyarrhythmias
|
Cardioversion
|
-Delivery of shock that is in synchrony with the QRS complex
-Purpose is to terminate dysrhythmias (PSVT, VT)
-An electrical shock during T wave can cause V-fib
|
A-Fib, atrial flutter
VT with a pulse
SVT
|
Defibrillation
|
-Delivery of a shock NOT in synchrony with QRS complex
-Purpose is to convert dysrhythmia to normal sinus rhythm
|
VT WITHOUT a pulse
V-fib
|
Automatic Implantable Defibrillator
|
Device that is surgically placed: when it detects a lethal dysrhythmia, it delivers a shock to defibrillate
Delivers a set number of shocks until the dysrhythmia is terminated
|
VT not controlled by medical therapy
V-fib
|
Pharmacologic Cardioversion
|
IV Ibutilide, Procainamide, Flecainide, Sotalol, Amiodarone
|
If electric cardioversion fails
|
Antiarrhythmics: “Some Bomb Pharmacology Class”
Class
|
Action
|
Indications
|
Contraindications
|
AE’s
|
Ia
|
Sodium channel blockers: higher affinity for open and/or inactivated state, slow down recovery
1. Decrease conduction velocity
2. Increase effective refractory period (slow transition from inactivated to resting, block re-entry circuits)
3. Raise threshold for impulse generation
|
SVT, V-tach
Prevention of V-fib
Symptomatic PVCs
|
MI, CAD
|
Quinidine (PO): Hypotension, diarrhea, thrombocytopenia, QT prolongation, SLE
Procainamide (IV): Hypotension, SLE
|
Ib
|
“ “
|
V-tach, prevention of V-fib
Symptomatic PVCs
|
HF, elderly
Lidocaine (cannot be used with corn allergy)
|
Lidocaine (IV): seizures, respiratory arrest, nervous, tremor, paresthesias
Mexiletine (PO): lightheaded, dizzy, nervous, ataxia, incoordination, tremor
|
Ic
|
“ “
|
Life-threatening V-tach or V-fib
Refractory SVT
Paroxysmal A-fib/Flutter
WPW
|
CHF, CAD - do not use in any heart abnormality
|
Flecainide: proarrhythmia, bronchospasm, leukopenia, thrombocytopenia, seizures
Black box: chronic A-fib
|
II
|
Beta-blockers: Block adrenergic receptors, blunting sympathetic effects
|
SVT, may prevent V-fib
|
Asthma, COPD
Bradycardia
AV block (chronic A-fib)
CHF/LVF
|
Esmolol
Propranolol: fatigue, impaired exercise, ED, chest pain, hypotension, bronchoconstriction, hypoglycemia
Metoprolol: bradycardia, impaired exercise, fatigue, ED, depression, chest pain
|
III
|
Potassium channel blockers
Blocks outward potassium channels, prolonging action potentials and increasing refractive period
Prolongs QT - monitor for QT prolongation
|
Refractory V-tach, ST
A-fib and flutter
Amiodarone: (IV) sustained VT, V-fib, (PO) A-fib, A-flutter, SVT, VT
Sotalol: A-fib
Dofetilide: A-fib, A-flutter
|
Amiodarone: pulmonary fibrosis, hypothyroidism, blue-gray skin, bradycardia, photosensitivity
Sotalol: bradycardia, bronchospasm, CHF, torsades
Dofetilide: liver injury, torsades
Ibutilide
| |
IV
|
CCB: affect SA and AV nodes
|
SVT
|
Verapamil, Diltiazem
| |
V
|
Adenosine: slows conduction time through AV node, interrupts reentry pathways
Digoxin: direct action on cardiac muscle and indirect action on CV system via ANS
|
SVT
|
Adenosine: headache, flush, SOB, chest pressure, nausea
Digoxin
|
Credits:
Dale Dubin
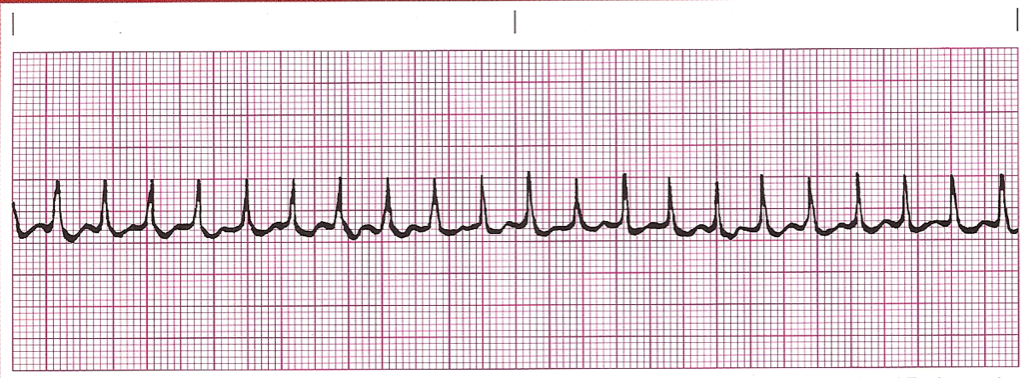
Question 1: A 76-year-old woman is hospitalized for altered mental status. Urinalysis shows >50 white blood cells per HPF and many bacteria. She is started on empiric antibiotics while urine cultures and sensitivities are pending. On the third day of hospitalization, she has an abnormal tracing on telemetry. Her past medical history is significant for myocardial infarction seven years ago and type II diabetes, for which she takes aspirin, metoprolol, lisinopril, metformin, and glipizide. Her pulse is 140 beats/minute, and blood pressure is 135/88 mm Hg. She is awake, alert, and fully oriented. She denies any lightheadedness, chest pain, or palpitations. A portion of her ECG is shown below. Which of the following is the next best step in the management of this patient?
- Adenosine
- Diltiazem
- Procainamide
- Transvenous pacing
- Unsynchronized cardioversion
Explanation:
The patient in this vignette has sustained monomorphic ventricular tachycardia (SMVT), which is defined by the following characteristics:
(1) Regular, wide QRS complex tachycardia at a rate of >100 beats/minute
(2) Consecutive beats have a stable QRS morphology
(3) Arrhythmia lasts ≥30 seconds or causes hemodynamic collapse
The treatment of SMVT depends on the degree of hemodynamic tolerance. For patients who are hemodynamically stable with SMVT, intravenous pharmacotherapy with an antiarrhythmic such as procainamide may be attempted prior to cardioversion. Amiodarone and sotalol have equal efficacy in terminated SMVT. Lidocaine has fallen out of favor due to less efficacy in comparison to the aforementioned drugs.
Answer A: Adenosine is used to diagnose and treat narrow QRS complex supraventricular tachycardia (SVT), not ventricular tachycardia.
Answer B: Diltiazem is incorrect. Diltiazem is a calcium channel blocker used for rate control in the atrial fibrillation with rapid ventricular response.
Answer D: Transvenous pacing is indicated in the case of severe bradyarrhythmias causing hemodynamic collapse.
Answer E: Patients with hemodynamically significant SMVT should be treated with immediate electrical cardioversion. Since this patient is asymptomatic, pharmacotherapy is the more appropriate initial step in management.
Bottom Line: Hemodynamically stable sustained monomorphic ventricular tachycardia is first treated with intravenous pharmacologic therapy (procainamide, amiodarone, sotalol, lidocaine), prior to electrical cardioversion.
Review the management of common arrhythmias, as they are frequently tested.
The patient in this vignette has sustained monomorphic ventricular tachycardia (SMVT), which is defined by the following characteristics:
(1) Regular, wide QRS complex tachycardia at a rate of >100 beats/minute
(2) Consecutive beats have a stable QRS morphology
(3) Arrhythmia lasts ≥30 seconds or causes hemodynamic collapse
The treatment of SMVT depends on the degree of hemodynamic tolerance. For patients who are hemodynamically stable with SMVT, intravenous pharmacotherapy with an antiarrhythmic such as procainamide may be attempted prior to cardioversion. Amiodarone and sotalol have equal efficacy in terminated SMVT. Lidocaine has fallen out of favor due to less efficacy in comparison to the aforementioned drugs.
Answer A: Adenosine is used to diagnose and treat narrow QRS complex supraventricular tachycardia (SVT), not ventricular tachycardia.
Answer B: Diltiazem is incorrect. Diltiazem is a calcium channel blocker used for rate control in the atrial fibrillation with rapid ventricular response.
Answer D: Transvenous pacing is indicated in the case of severe bradyarrhythmias causing hemodynamic collapse.
Answer E: Patients with hemodynamically significant SMVT should be treated with immediate electrical cardioversion. Since this patient is asymptomatic, pharmacotherapy is the more appropriate initial step in management.
Bottom Line: Hemodynamically stable sustained monomorphic ventricular tachycardia is first treated with intravenous pharmacologic therapy (procainamide, amiodarone, sotalol, lidocaine), prior to electrical cardioversion.
Review the management of common arrhythmias, as they are frequently tested.
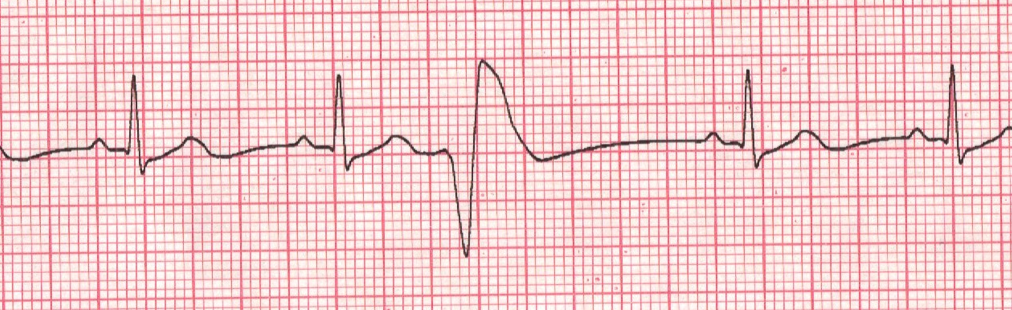
Question 2: A 50-year-old African American woman comes to the emergency room with a vague feeling of discomfort. She denies any loss of consciousness, chest pain, or diaphoresis. She has been compliant with her metoprolol and hydrochlorothiazide but has had decreased exercise tolerance. The physical examination is normal, except for mild edema bilaterally in each ankle. A portion of her ECG is shown below. Which of the following treatments is best for the following arrhythmia?
A. Atropine
B. Adenosine
A. Atropine
B. Adenosine
C. Amiodarone
D. Electrical cardioversion
E. Pacemaker placement
Explanation:
The above rhythm strip shows a Mobitz type 2 heart block. This rhythm has a fixed PR interval with the occasional dropped beat. This beat can progress to complete heart block, so the patient must be monitored closely in an ICU until a pacemaker can be implanted.
Answer A: Atropine is used in resuscitation of a patient with bradycardia and asystole since it blocks acetylcholine and provides sympathetic stimulation to the heart.
Answer B: Adenosine is used for patients with SVT since it acts on the AV node to stop any reentrant circuit.
Answer C: Amiodarone is an anti-arrhythmic agent with a significant side effect profile. There is no need for an anti-arrhythmic in this case, as pacemaker is definitive treatment.
Answer D: Electrical Cardioversion is always used in patients who are unstable with an arrhythmia or who are in ventricular fibrillation or tachycardia. This patient has a block, which does not respond to cardioversion.
Bottom Line: Mobitz type II blocks consist of a fixed PR interval with dropped QRS complexes. Treatment of Mobitz II block always requires pacemaker placement due to possible progression to complete block.
D. Electrical cardioversion
E. Pacemaker placement
Explanation:
The above rhythm strip shows a Mobitz type 2 heart block. This rhythm has a fixed PR interval with the occasional dropped beat. This beat can progress to complete heart block, so the patient must be monitored closely in an ICU until a pacemaker can be implanted.
Answer A: Atropine is used in resuscitation of a patient with bradycardia and asystole since it blocks acetylcholine and provides sympathetic stimulation to the heart.
Answer B: Adenosine is used for patients with SVT since it acts on the AV node to stop any reentrant circuit.
Answer C: Amiodarone is an anti-arrhythmic agent with a significant side effect profile. There is no need for an anti-arrhythmic in this case, as pacemaker is definitive treatment.
Answer D: Electrical Cardioversion is always used in patients who are unstable with an arrhythmia or who are in ventricular fibrillation or tachycardia. This patient has a block, which does not respond to cardioversion.
Bottom Line: Mobitz type II blocks consist of a fixed PR interval with dropped QRS complexes. Treatment of Mobitz II block always requires pacemaker placement due to possible progression to complete block.
Question 3: A 67-year-old man presents to the emergency department with lightheadedness. He denies chest pain, palpitations, sweating, nausea, vomiting or diarrhea. He has a long standing history of hypertension. His extremities are cool, distal digits and oral mucosa have a grayish hue. His radial pulses are weak. His ECG is shown below. Which of the following is the most appropriate next step in the management of this patient?
A. Atropine
B. Defibrillation
C. Discontinue medication
D. Transcutaneous pacing
E. Transvenous pacing
Explanation:
Sinus bradycardia is defined by the presence of ventricular heart rate < 60 beats/minute, regular rhythm, and constant PR intervals on ECG. Most patients are asymptomatic; however, a patient with symptomatic sinus bradycardia may complain of dizziness or lightheadedness, syncope, dyspnea, and chest pain. Sinus bradycardia is associated with excellent physical conditioning, sick sinus syndrome, hypoglycemia, medications (calcium channel blockers, beta blocker and digoxin) and structural heart disease. Sinus bradycardia may also be seen with hypothermia and hypoglycemia.
Atropine is indicated in the treatment of hemodynamically unstable sinus bradycardia with evidence of hypoperfusion, manifested in this patient as pale dusky extremities and weak peripheral pulses.
Answer B: Defibrillation is indicated in patients with hemodynamically significant ventricular tachycardia and in ventricular fibrillation with or without palpable pulses.
Answer C: This patient’s medications are not given, and only discontinuing a possible offending agent responsible for his bradycardia without other intervention would not be appropriate given his acute, compromising symptoms.
Answer D: A temporary transcutaneous pacemaker is the next appropriate step should the patient remain symptomatic and with continued evidence of hypoperfusion, but atropine should be attempted first.
Answer E: Transvenous pacing is an invasive procedure that should not be attempted prior to pharmacologic management in an awake, alert patient with no contraindications for atropine.
Bottom Line: Symptomatic bradycardia with signs of hypoperfusion is first treated with atropine.
A. Atropine
B. Defibrillation
C. Discontinue medication
D. Transcutaneous pacing
E. Transvenous pacing
Explanation:
Sinus bradycardia is defined by the presence of ventricular heart rate < 60 beats/minute, regular rhythm, and constant PR intervals on ECG. Most patients are asymptomatic; however, a patient with symptomatic sinus bradycardia may complain of dizziness or lightheadedness, syncope, dyspnea, and chest pain. Sinus bradycardia is associated with excellent physical conditioning, sick sinus syndrome, hypoglycemia, medications (calcium channel blockers, beta blocker and digoxin) and structural heart disease. Sinus bradycardia may also be seen with hypothermia and hypoglycemia.
Atropine is indicated in the treatment of hemodynamically unstable sinus bradycardia with evidence of hypoperfusion, manifested in this patient as pale dusky extremities and weak peripheral pulses.
Answer B: Defibrillation is indicated in patients with hemodynamically significant ventricular tachycardia and in ventricular fibrillation with or without palpable pulses.
Answer C: This patient’s medications are not given, and only discontinuing a possible offending agent responsible for his bradycardia without other intervention would not be appropriate given his acute, compromising symptoms.
Answer D: A temporary transcutaneous pacemaker is the next appropriate step should the patient remain symptomatic and with continued evidence of hypoperfusion, but atropine should be attempted first.
Answer E: Transvenous pacing is an invasive procedure that should not be attempted prior to pharmacologic management in an awake, alert patient with no contraindications for atropine.
Bottom Line: Symptomatic bradycardia with signs of hypoperfusion is first treated with atropine.
No comments:
Post a Comment
Leave a comment with feedback, questions, or inquiries for Paul. He will try to respond within 1-2 weeks.