Antibiotics for Physician Assistants - Part I
Updated: 08/07/2016
- Empiric therapy is defined as the initiation of treatment prior to firm diagnosis, and knowing the specific organism causing the infection
- Started only after cultures have been obtained
- Targets likely pathogens and must use local antibiogram
- Broad spectrum means covering both gram positive and gram negative bacteria
- Pharmacokinetics: what the body does to a drug
- Absorption: described in terms of bioavailability (F)
- 100% bioavailable drugs (PO = IV): Linezolid, Fluoroquinolones, Tetracyclines, Azithromycin, Metronidazole, Trimethoprim/Sulfamethoxazole (Bactrim), Rifampin
- Distribution: affected by protein binding, blood flow, molecular size, lipophilicity, inflammation, and fluid status
- Metabolism: occurs primarily in the liver via multiple mechanisms
- Phase I: oxidation/reduction (CYP 450), hydrolysis
- Phase II: glucuronidation, sulfonation, methylation, acetylation, glutathione
- Elimination: primarily renal (glomerular filtration and tubular secretion)
- Most antibiotics require dose adjustment for creatinine clearance (CrCl) <50 mL/min

Cell Wall Synthesis Inhibitors
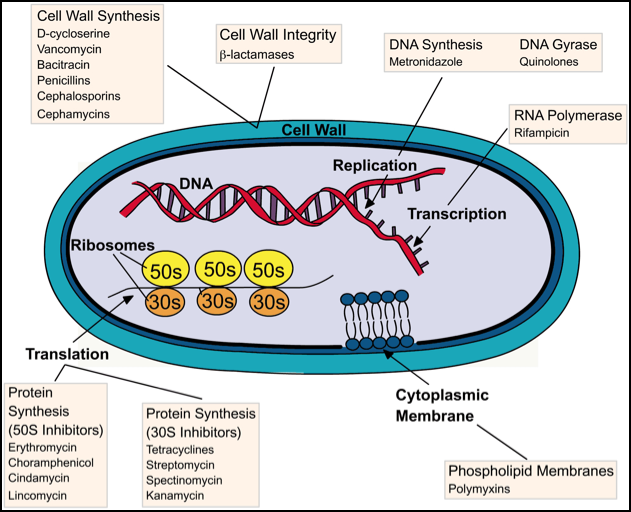
(Penicillins, Cephalosporins, and Carbapenems)
Penicillins
- MOA: binds to penicillin binding proteins on surface of cell wall and inhibits cell wall synthesis
- Variable PO absorption, short half lives (frequent dosing), primarily renally eliminated
Indications
|
Dose
|
Pearls
| |
Penicillin G
|
Streptococcal infections
Syphilis
Staph aureus (susceptible)
|
IM/IV: 3-4 million units q 4 hours
|
Continuous infusion over 24 hours if normal renal function
|
Penicillin G Benzathine
|
Syphilis
|
IM: 2.4 million units x 1 (primary, secondary, early latent)
IM: 2.4 million units weekly (late latent, latent of unknown duration)
|
IM injection
Longer acting
|
Penicillin V Potassium (VK)
|
Actinomycosis
Erysipelas
Streptococcal Pharyngitis
|
PO: 250-500 mg q 6 hours
| |
Anti-staphylococcus or Penicillinase Resistant
Oxacillin (IV), Nafcillin (IV), Dicloxacillin (PO)
|
Methicillin-susceptible staph aureus (MSSA)
Narrow spectrum gram (+) coverage
Staphylococcal skin/soft tissue infections (mastitis)
|
2 grams q 4 hours
|
Continuous infusion over 24 hours if normal renal function
May increase warfarin requirement (drop INR)
|
Aminopenicillins: gram negative and positive coverage
Indications
|
Dose
|
Pearls
| |
Ampicillin
|
E. coli
Proteus (K. pneumoniae intrinsically resistant)
Listeria
Enterococcus: gram (+) cocci in pairs; faecalis
Streptococcus: gram (+), viridans, pyogenes, pneumoniae, agalactiae
|
IV: 2 grams q 4-6 hours
PO:
|
Gram positive and negative coverage (limited)
|
Ampicillin/Sulbactam
[Unasyn]
|
Similar to Ampicillin
Better Gram (-) coverage
Acinetobacter
Anaerobes: E. coli
Skin/soft tissue infections, intraabdominal and peritonitis
|
IV: 3 grams q 4-6 hours
| |
Amoxicillin
|
Similar to Ampicillin
UTI in pregnancy, AOM
|
PO: 500-1000 mg q 8-12 hours
|
Lower bioavailability than IV ampicillin (greater than PO ampicillin)
Gram positive and negative coverage (limited)
|
Amoxicillin/
Clavulanate [Augmentin]
|
Similar to Amoxicillin
Better Gram (-) coverage
Anaerobes (not Acinetobacter): E. coli, Salmonella, Shigella, Campylobacter, H. pylori, Klebsiella
AOM, sinusitis, dental infections, bites
|
PO: 250-500 q 8 hours OR
PO: 875 mg q 12 hours
|
Antipseudomonal Penicillins
Indications
|
Dose
|
Pearls
| |
Piperacillin/
Tazobactam (Zosyn)
|
MSSA
Empiric or definitive therapy for Pseudomonas aeruginosa
Anaerobes
Enterococcus: gram (+) cocci in pairs; faecalis
Streptococcus: gram (+), viridans, pyogenes, pneumoniae, agalactiae
|
IV: 3.375-4.5 g q 6-8 hours
|
Can be given extended infusion (over 4 hours) or continuous infusion
Zosyn and Cefepime are the empiric broad spectrum agents of choice at most institutions
No atypical coverage (Legionella, Mycoplasma, Chlamydia)
|
Cephalosporins
- As you increase generation, you generally add greater gram negative coverage, but lose gram positive coverage
- Cross-reactivity in patients with penicillin allergy: 10%
- If patient has had true IgE mediated (anaphylaxis) reaction, avoid all B-lactams including Carbapenems (Exception: can give aztreonam)
Indications
|
Dose
|
Pearls
| |
First Generation
Cefazolin (Ancef)
Cephalexin (Keflex)
|
Staphylococcus: aureus, epidermidis, haemolyticus, saprophyticus
Streptococcus: gram (+), viridans, pyogenes, pneumoniae, agalactiae
Aerobic GRN: M. catarrhalis, E. coli, K. pneumoniae
Skin and soft tissue infections, surgical prophylaxis,
ENT: Streptococcal pharyngitis
GU: UTI
Pediatric osteomyelitis
|
IV: Cefazolin 1-2 g IV q 8 hours
PO: Cephalexin 250-500 mg q 6 hours (good absorption)
|
No CSF penetration
|
Second Generation
Cefuroxime (Ceftin PO, Zinacef IV/IM)
Cefoxitin (Mefoxin)
|
Aerobic GNR: H. flu, M. cat, N. meningitidis
Anaerobes: E. coli
Skin/soft tissue infections
GU: UTI
Pulm: Mild CAP (3rd Gen preferred), acute chronic bronchitis exacerbation
ENT: sinusitis, AOM
Surgical prophylaxis (GI/GU)
Abdominal infections
|
PO: Cefuroxime axetil 250-500 mg q 12 hours
IV: Cefuroxime 1.5 g q 8 hours
IV: Cefoxitin 1-2 grams q 4-6 hours
| |
Third Generation
Ceftriaxone (Rocephin)
Cefotaxime (Claforan)
Ceftazidime (Fortaz, Tazicef)*
|
Improved Anaerobic GNR: E. coli, Klebsiella, P. mirabilis, S. pneumoniae
MSSA coverage
*Ceftazidime: Pseudomonas
Ceftriaxone: Meningitis
Gonorrhea, CAP
|
IV/IM: Ceftriaxone 1-2 g q 24 hours (2 g q 12 for meningitis)
IV: Cefotaxime 1-2 g q 4-8 hours
IV: Ceftazidime 1-2 g q 8 hours
|
Ceftriaxone - good CNS penetration (higher dose)
|
Fourth Generation
Cefepime (Maxipime)
|
Empiric or definitive therapy against Pseudomonas aeruginosa
Febrile neutropenia
|
IV: 1-2 grams q 8-12 hours
|
Unlike Zosyn, no anaerobic or enterococcus activity
Less gram positive coverage than lower generations
|
Fifth Generation
Ceftaroline (Teraflo, Zinforo)
|
GN coverage similar to ceftriaxone
Streptococcus
Staphylococcus (MRSA)
|
IV: 600 mg q 8-12 hours
|
Monobactams
Aztreonam
|
Gram negative only
Pseudomonas
|
IV: 2 grams q 6-8 hours
|
No cross-reactivity with other beta-lactams
|
Carbapenems
Ertapenem
|
Gram negative coverage: ESBL producing Enterobacteriaceae
Streptococcus
MSSA
Anaerobes
|
IV: 1 g q 24 hours
| |
Meropenem
|
Same as Ertapenem
Pseudomonas aeruginosa
Acinetobacter
Enterococcus
|
IV: 1 g q 8 hours
IV: 2 g q 8 hours (CNS)
|
Broad spectrum activity, limit activity
|
Imipenem/Cilastatin
Primaxin
|
Similar to Meropenem
Nocardia
Nontuberculous mycobacterial organisms
|
IV: 500 mg q 6 hours
|
Imipenem is rapidly inactivated by renal dehydropeptidase I (DHP-1), cilastatin is a DHP-1 inhibitor that allows for a prolonged half life and increased tissue penetration
|
Adverse Effects of Beta Lactams
- Hypersensitivity
- Cross reactivity of cephalosporins is <10%
- Avoid all beta-lactams for anaphylactic reactions, including carbapenems
- Exception: can give aztreonam
- Seizures: higher risk with carbapenems
- Highest when not renally-dosed
- Nafcillin, oxacillin, and ceftriaxone - only beta-lactams that do not require renal adjustment
- Electrolyte Imbalance (Na and K): most often with salts (penicillin G potassium or nafcillin sodium)
Other Bacterial Cell Wall Agents
- Binds to the D-ala-D-ala terminus of the peptidoglycan molecule preventing cross linking of the chains by penicillin binding protein → weakens cell wall and causes osmotic lysis
Vancomycin
(Vancocin)
|
Aerobic gram (+): MRSA, MSSA, S. pneumoniae
Anaerobic gram (+)
Empiric therapy when MRSA suspected, MDRS in CA meningitis, severe infections with MRSA, CoNS, Enterococcus resistant to ampicillin
Sepsis, meningitis, pneumonia, infective endocarditis
|
Loading dose of 25 mg/kg in critically ill patients
Maintenance dose: 15 mg/kg based on TBW
Frequency based on renal function (most q 12)
|
No gram (-) activity
PO formulation for C. difficile due to poor absorption
Bactericidal, slower than B-lactams
Bacteriostatic against Enterococcus
Trough levels used to determine efficacy and nephrotoxicity (goal: 15-20)
SCr: baseline and every 3-4 days
|
Bacitracin
(BACiiM, Bacitracin)
|
Gram (+) and Gram (-) activity
Staphylococcal pneumonia, aureus, epidermidis
Streptococcus pyogenes
|
IM
Topical
|
Decreased incidence of cross reaction with sulfa drugs when not combined with polymyxin B and neomycin
|
Cyclic Lipopeptide
- Calcium-dependent insertion of lipid tail leading to disruption of cell membrane and cell death
Daptomycin
(Cubicin)
|
MDRS and gram (+)
MRSA, MSSA, VRE, S. pneumoniae, another streptococcal spp.
Must have failed or had intolerant response to vancomycin
|
IV (skin/soft tissue): 4 mg/kg daily
All other: 6-8 mg/kg daily, based on TBW
|
No gram negative activity
Not for use in pneumonia (lung surfactant binds the drug)
Monitor CPK at baseline and weekly
|
Phospholipid Membrane Inhibitor
- MOA: Bind to outer membrane of GN bacteria leading to disruption of membrane instability and leakage of cellular contents
Polymyxin
Colistin (colistimethate sodium)
|
Highly resistant GNR, including Pseudomonas and Klebsiella
Acinetobacter
CRE: Carbapenem resistant Enterobacteriaceae
Multidrug resistant GN infections: pneumonia, bacteremia, sepsis, complicated UTIs
|
IM, IV
Ophthalmic
Topical
|
Poor gram (+) coverage and anaerobic coverage
|
Question 1: What determines if a bacterial organism is gram negative or gram positive?
Question 2: Why isn’t a beta lactam antibiotic or other agent that inhibits cell wall synthesis used for young healthy people with community acquired pneumonia?
Question 3: Which of the following antibiotics provides the best activity against gram negative bacteria?
- Daptomycin (Cubicin)
- Clindamycin (Cleocin)
- Rifampin
- Aztreonam
Question 4: Which pair of medications does not have cross-reactivity?
- Linezolid and SSRIs
- Aztreonam and Penicillin G
- Daptomycin and Statin
- Erythromycin and Warfarin
Answer 1: Gram positive organisms have a peptidoglycan layer
- Gram negative organisms have a thick polysaccharide layer
Answer 2: Atypicals do not have a cell wall
Answer 3: D, the rest have gram positive coverage
Answer 4: B, both are Beta lactams
No comments:
Post a Comment
Leave a comment with feedback, questions, or inquiries for Paul. He will try to respond within 1-2 weeks.